- Epidemiology & Risk Factors
- Congenital vascular anomaly; most common symptomatic vascular ring.
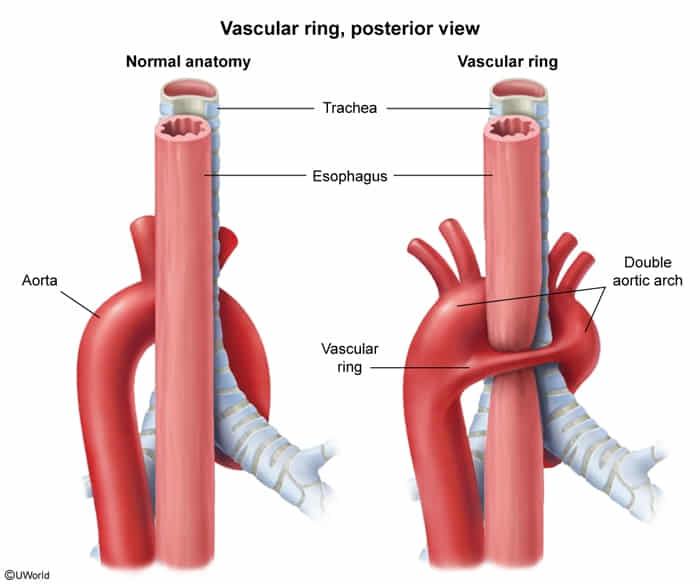
- Pathophysiology: Persistence of both right and left embryonic 4th aortic arches, encircling the trachea and esophagus.
- Usually sporadic/isolated anomaly (unlike other arch anomalies which may be strongly a/w DiGeorge syndrome/22q11.2 deletion).
- Clinical Features
- Tracheal + Esophageal compression (complete vascular ring).
- Presentation usually in early infancy (< 6 months).
- Resp: Biphasic stridor (worsens w/ crying, feeding, or supine pos), chronic cough, wheezing, recurrent resp infections. c
- GI: Dysphagia to solid foods (in older infants), vomiting/choking w/ feeds, FTT.
- Positioning: Infant often assumes a neck hyperextension posture to relieve tracheal compression; neck flexion exacerbates stridor.
- Diagnosis
- Initial:
- CXR: May show narrowed trachea or right-sided aortic arch.
- Barium swallow: High-yield screening tool showing classic bilateral indentations on the esophagus.
- Echocardiogram: To rule out associated intracardiac defects.
- Confirmatory/Gold Standard: CTA or MRA of the chest. Provides definitive 3D mapping of the vascular anatomy for surgical planning.
- Adjunct: Bronchoscopy/Endoscopy (reveals pulsatile extrinsic compression of the trachea/esophagus).