-
Epidemiology & Risk Factors
- Most common congenital nasal anomaly.
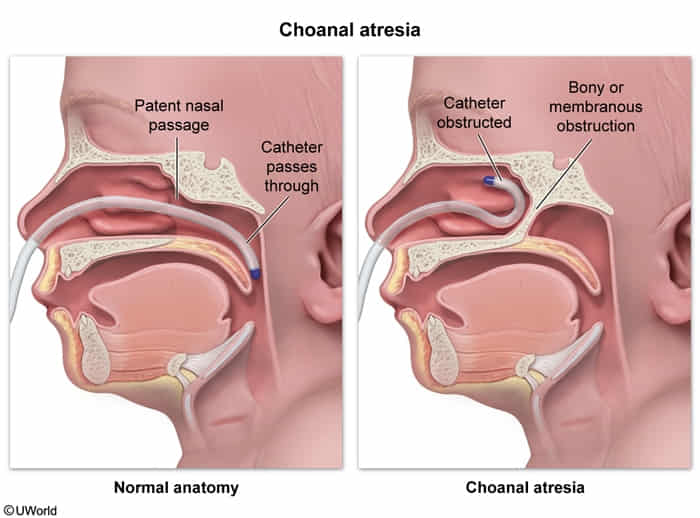
- Pathophysiology: Failure of posterior nasal passage (choanae) to canalize (can be bony, membranous, or mixed).
- Highly associated with CHARGE syndrome: Coloboma, Heart defects, Atresia choanae, Retardation of growth/development, GU anomalies, Ear anomalies/deafness.
-
Clinical Features
- Bilateral (Neonatal presentation):
- Neonates are obligate nasal breathers.
- Paradoxical cyanosis: Cyanosis/resp distress that worsens with sleeping or feeding, and improves with crying (as the mouth opens).
- Noisy breathing (stertor) and feeding difficulties.
- Unilateral (Childhood presentation):
- Often asymptomatic at birth.
- Presents later with chronic, purulent, or mucoid unilateral nasal discharge.
- Bilateral (Neonatal presentation):
-
Diagnosis
- Initial/Screening: Inability to pass a small catheter (e.g., 8-10F) through the nares into the oropharynx.
- Confirmatory/Gold Standard: CT scan of the facial bones/paranasal sinuses (delineates bony vs. membranous obstruction and narrows surgical approach).
- Adjunct: Rigid nasal endoscopy (visualizes obstruction).
- Initial/Screening: Inability to pass a small catheter (e.g., 8-10F) through the nares into the oropharynx.
-
Differential Diagnostics
- Cyanotic Congenital Heart Disease (e.g., Tetralogy of Fallot): Diff by cyanosis worsening with crying (Tet spells), abnormal cardiac auscultation (murmurs), and abnormal ECG/Echo.
- Tracheoesophageal Fistula (TEF) / Esophageal Atresia: Diff by choking/coughing with feeding, but no paradoxical improvement with crying. Catheter passes through nose but coils in the esophagus.
- Nasal Foreign Body: Diff by acute/subacute onset of unilateral foul-smelling purulent discharge in a toddler/older child; visualized directly on rhinoscopy.
-
Management
- Stabilize (Bilateral): Immediate airway security is priority. Place an oral airway, McGovern nipple, or perform endotracheal intubation if severe resp distress.
- Supportive: Orogastric (OG) tube placement for feeding.
- Definitive: Surgical repair (endoscopic transnasal puncture/resection w/ or w/o stenting).
-
Complications
- Asphyxiation / Respiratory arrest (if bilateral).
- Aspiration pneumonia.
- Failure to thrive (FTT) due to feeding difficulties.
- Post-operative restenosis.