-
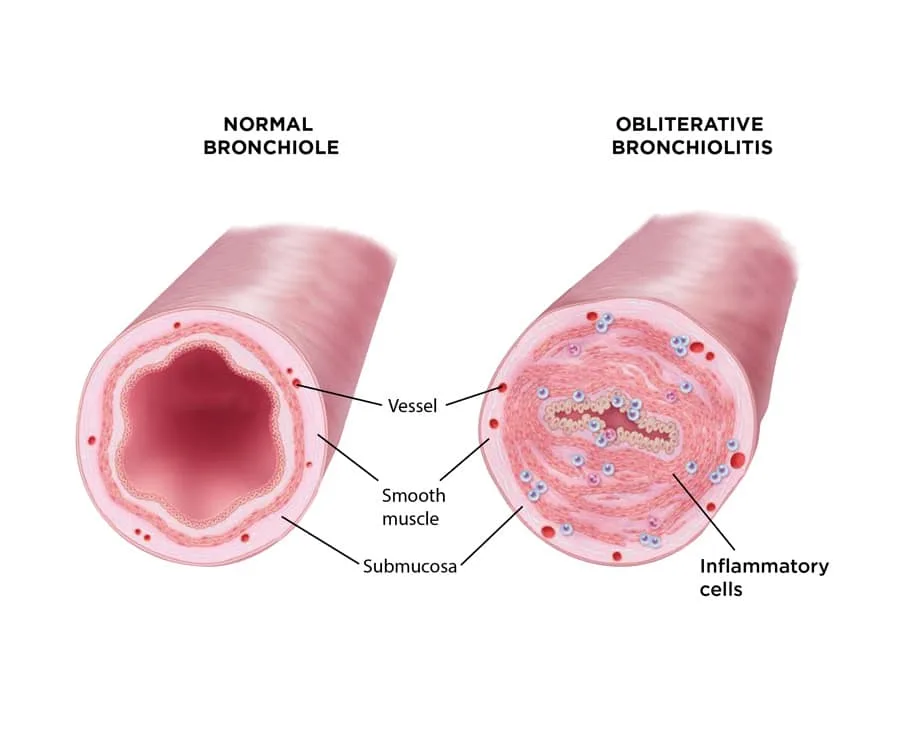
Submucosal fibrosis leads to concentric narrowing of the bronchiolar lumen.
-
Progressive scarring eventually results in complete closure (obliteration) of the small airways.
-
Epidemiology & Risk Factors
- Lung Transplant: The hallmark of chronic allograft rejection (occurs months to years post-transplant; leading cause of long-term mortality). c
- Hematopoietic Stem Cell Transplant (HSCT): Manifestation of chronic Graft-Versus-Host Disease (GVHD).
- Toxic Inhalation: Diacetyl (“popcorn lung” in microwave popcorn factory workers), nitrogen dioxide (silo filler’s disease), sulfur mustard, chlorine gas.
- Post-Infectious: Severe viral infections in childhood (RSV, Adenovirus) or atypical pneumonia (Mycoplasma).
- Autoimmune: Rheumatoid Arthritis (RA).
-
Clinical Features
- Insidious onset of progressive dyspnea on exertion (DOE).
- Dry, nonproductive cough.
- Wheezing and end-inspiratory squeaks/crackles on auscultation.
- Key Feature: Symptoms are not reversible with bronchodilators.
-
Diagnosis
- Initial/Screening: Pulmonary Function Tests (PFTs).
- Shows a fixed obstructive pattern: ↓ FEV1, ↓ FEV1/FVC (< 70%). c
- Negative bronchodilator response.
- Normal DLCO (helps differentiate from emphysema).
- Imaging:
- CXR: Often normal or shows hyperinflation.
- High-Resolution CT (HRCT): Test of choice. Shows mosaic attenuation (patchy areas of relative lucency), expiratory air trapping, and bronchial wall thickening.
- Confirmatory/Gold Standard: Lung biopsy.
- Definitive diagnosis but often unnecessary if clinical context (e.g., post-transplant) and HRCT are classic.
- Histology: Submucosal fibroproliferation leading to concentric narrowing/obliteration of membranous and respiratory bronchioles.
- Initial/Screening: Pulmonary Function Tests (PFTs).
-
Differential Diagnostics
- Asthma: Diff by (+) bronchodilator reversibility on PFTs and episodic nature.
- COPD/Emphysema: Diff by smoking hx and ↓ DLCO.
- Bronchiectasis: Diff by chronic productive (purulent) cough, hemoptysis, and marked airway dilation/signet ring sign on HRCT.
- Cryptogenic Organizing Pneumonia (COP/BOOP): Diff by restrictive PFT pattern, alveolar infiltrates on imaging, and rapid response to systemic corticosteroids.
-
Management
- Primary/Supportive: Discontinue offending exposures. Supplemental O2, symptom management (inhaled bronchodilators, cough suppressants), and pulmonary rehab.
- Post-Transplant/GVHD: Augment systemic immunosuppression (e.g., tacrolimus, cyclosporine, systemic steroids).
- Adjunctive: Macrolides (e.g., Azithromycin) often used for immunomodulatory and anti-inflammatory properties (↓ IL-8).
- Refractory/Definitive: Re-transplantation for severe, progressive disease.
-
Complications
- Progressive, irreversible respiratory failure.
- Cor pulmonale (right heart failure 2/2 pulmonary HTN).
- Increased susceptibility to secondary respiratory infections.