Laryngomalacia
- Epidemiology & Risk Factors
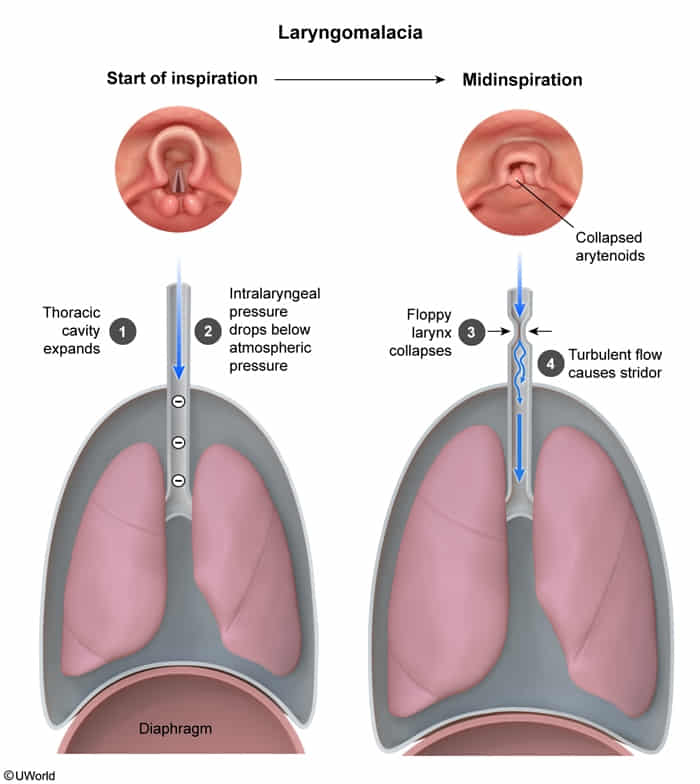
- Most common cause of stridor in infants.
- Presentation typically begins at 1-2 weeks of age.
- Peaks at 4-8 months; resolves spontaneously by 12-18 months in >90% of pts.
- Strongly associated w/ GERD.
- Clinical Features
- Inspiratory stridor: Worsens w/ crying, feeding, agitation, or supine position. Improves when prone.
- Normal phonation/cry (differentiates from vocal cord pathologies).
- Feeding difficulties (choking, coughing, regurgitation).
- Severe cases: Cyanosis, apnea, retractions.
- Diagnosis
- Initial/Screening: Often a clinical diagnosis based on classic H&P.
- Confirmatory/Gold Standard: Flexible laryngoscopy in an awake infant.
- Classic findings: Collapse of supraglottic structures during inspiration, shortened aryepiglottic folds, omega-shaped (Ω) epiglottis.
- Imaging: X-rays typically not required but may show concurrent conditions (e.g., fluoroscopy/barium swallow if vascular ring suspected).
- Differential Diagnostics
- Tracheomalacia: Diff by expiratory stridor; intrathoracic airway collapse. Worsens w/ forced expiration (crying, coughing).
- Vascular Ring: Diff by biphasic stridor that improves w/ neck extension. Often accompanied by dysphagia (esophageal compression).
- Vocal Cord Paralysis: Diff by weak cry, hoarseness, biphasic stridor. Hx of difficult delivery or cardiothoracic surgery.
- Subglottic Stenosis: Diff by biphasic stridor, Hx of prolonged intubation (acquired) or failed extubation.
- Management
- First-line (Mild/Moderate): Reassurance & observation. Upright feeding.
- Medical: Acid suppression (PPIs/H2 blockers) if concurrent GERD is present (GERD exacerbates supraglottic swelling and collapse).
- Surgical (Severe): Supraglottoplasty. Indicated ONLY for severe symptoms:
- Failure to thrive (FTT) / poor weight gain.
- Apnea or cyanotic episodes.
- Cor pulmonale.
- Complications
- Failure to thrive (2° to increased work of breathing and feeding difficulties).
- Obstructive sleep apnea (OSA).
- Pulmonary HTN / Cor pulmonale (rare, in severe untreated cases).
- Aspiration.