Herniation of pelvic organs (bladder, uterus, rectum, vaginal apex) into or out of the vagina due to weakened pelvic floor muscles and connective tissue.
Epidemiology
Etiology
- Etiology: insufficiency of the pelvic floor muscles and the ligamentous supportive structure of the uterus and vagina
- Risk factors:
- Multiple vaginal deliveries and/or traumatic births (greatest risk factor)
- Low estrogen levels (e.g., during menopause)
- Increased intraabdominal pressure (due to, e.g., obesity, cough related to chronic lung disease and/or smoking, ascites, pelvic tumors, constipation)
Pathophysiology
| Type | Defect | Key Association |
|---|---|---|
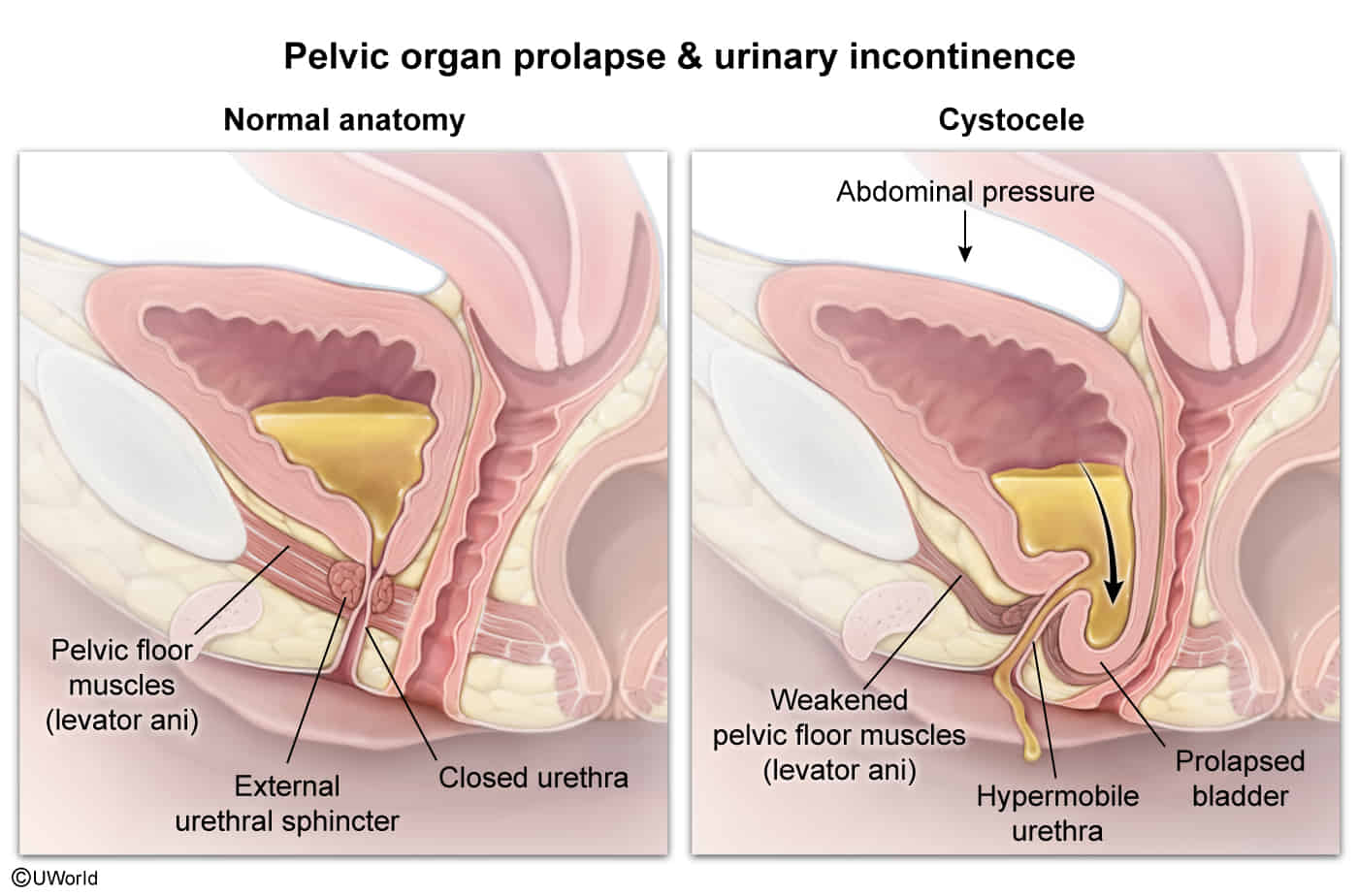
| Cystocele | Anterior (Bladder) t | Urinary Sx (incontinence, retention) |
| Rectocele | Posterior (Rectum) | Constipation; “Splinting” to defecate |
| Enterocele | Small bowel (Pouch of Douglas) | Post-hysterectomy; apical bulge |
| Apical | Cardinal/Uterosacral ligs | Cervix at introitus; “Sitting on a ball” |
- Specific sites
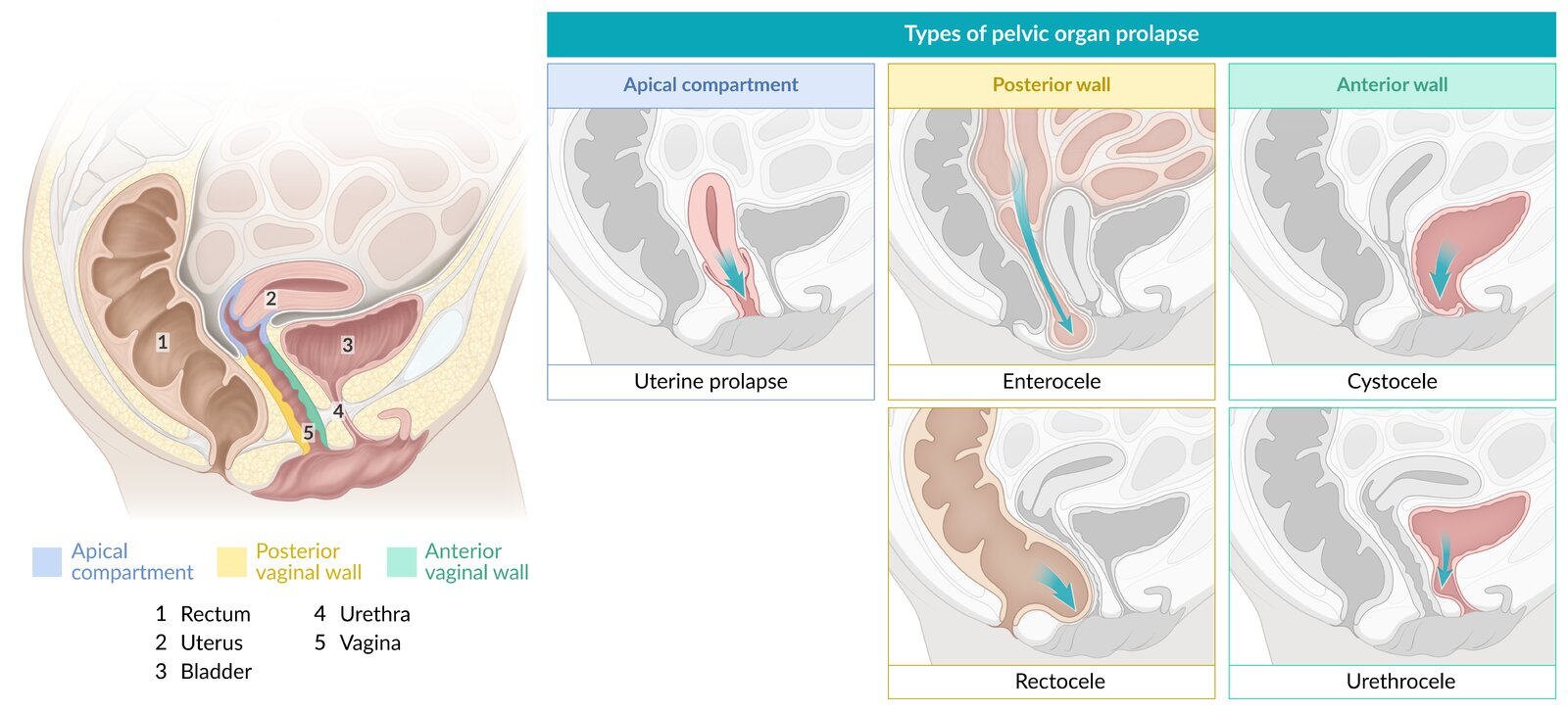
- Vaginal wall prolapse
- Anterior vaginal wall prolapse: herniated anterior vaginal wall, which is often associated with a cystocele (descent of the bladder) or urethrocele (descent of the urethra); can be due to weakness of the pubocervical fascia; Most common type.
- Posterior vaginal wall prolapse: herniated posterior vaginal wall, which is associated with a rectocele (descent of the rectum) or enterocele (herniated section of the intestines); can be due to weakness of the rectovaginal fascia
- Uterine prolapse: descent of the uterus
- Vaginal vault prolapse: descent of the apex of the vagina
- Apical compartment prolapse: herniated uterus, cervix, or vaginal vault
- Uterine procidentia: protrusion of all vaginal walls or cervix beyond the vaginal introitus
- Vaginal wall prolapse
Clinical features
- Feeling of pressure on or discomfort around the perineum (“sensation of vaginal fullness”)
- Lower back and pelvic pain (may become worse with prolonged standing or walking)
- Rectal fullness, constipation, incomplete rectal emptying
- Prolapse of the anterior (most common) or the posterior vaginal wall
- Weakened pelvic floor muscle and anal sphincter tone
Diagnostics
Treatment
- Treatment is guided by symptom severity and patient preference. Asymptomatic prolapse often requires no intervention.
- Conservative Management (First-line for mild/moderate symptoms):
- Pelvic floor muscle training (PFMT) / Kegel exercises: Strengthens the levator ani muscles.
- Vaginal pessary: A removable silicone device inserted into the vagina to provide structural support. Requires periodic cleaning.
- Vaginal estrogen: Topical creams/rings can improve tissue atrophy, especially in postmenopausal women.
- Lifestyle modification: Weight loss, treatment of chronic cough/constipation.
- Surgical Management (For severe, symptomatic prolapse or failure of conservative Tx):
- Reconstructive procedures: Apical suspension (e.g., sacrocolpopexy, uterosacral ligament suspension) or anterior/posterior colporrhaphy (repair of specific vaginal walls).
- Obliterative procedures (Colpocleisis): Vagina is surgically closed. Reserved for elderly, non-sexually active patients with significant comorbidities.
- Hysterectomy may be performed concurrently with prolapse repair.