Ovarian cancer
Epidemiology
- Incidence
- Second most common gynecological cancer (after endometrial cancer)
- Incidence increases with age
- Age
- Peak incidence: 55–64 years of age
Etiology
The most likely pathogenesis of EOC is repeated injury and repair to the ovarian surface, which makes surface epithelial cells susceptible to malignant transformation (ie, acquiring oncogenic mutations).
Risk factors
- Hormonal factors
- Elevated number of ovulatory cycles: early menarche and/or late menopause
- Nulliparity
- Endometriosis
Protective factors
- Combined oral contraceptive pills
- Multiparity
- Breastfeeding
- Bilateral salpingo-oophorectomy
- Bilateral tubal ligation
- Hysterectomy
Pathophysiology
Clinical features
Tip
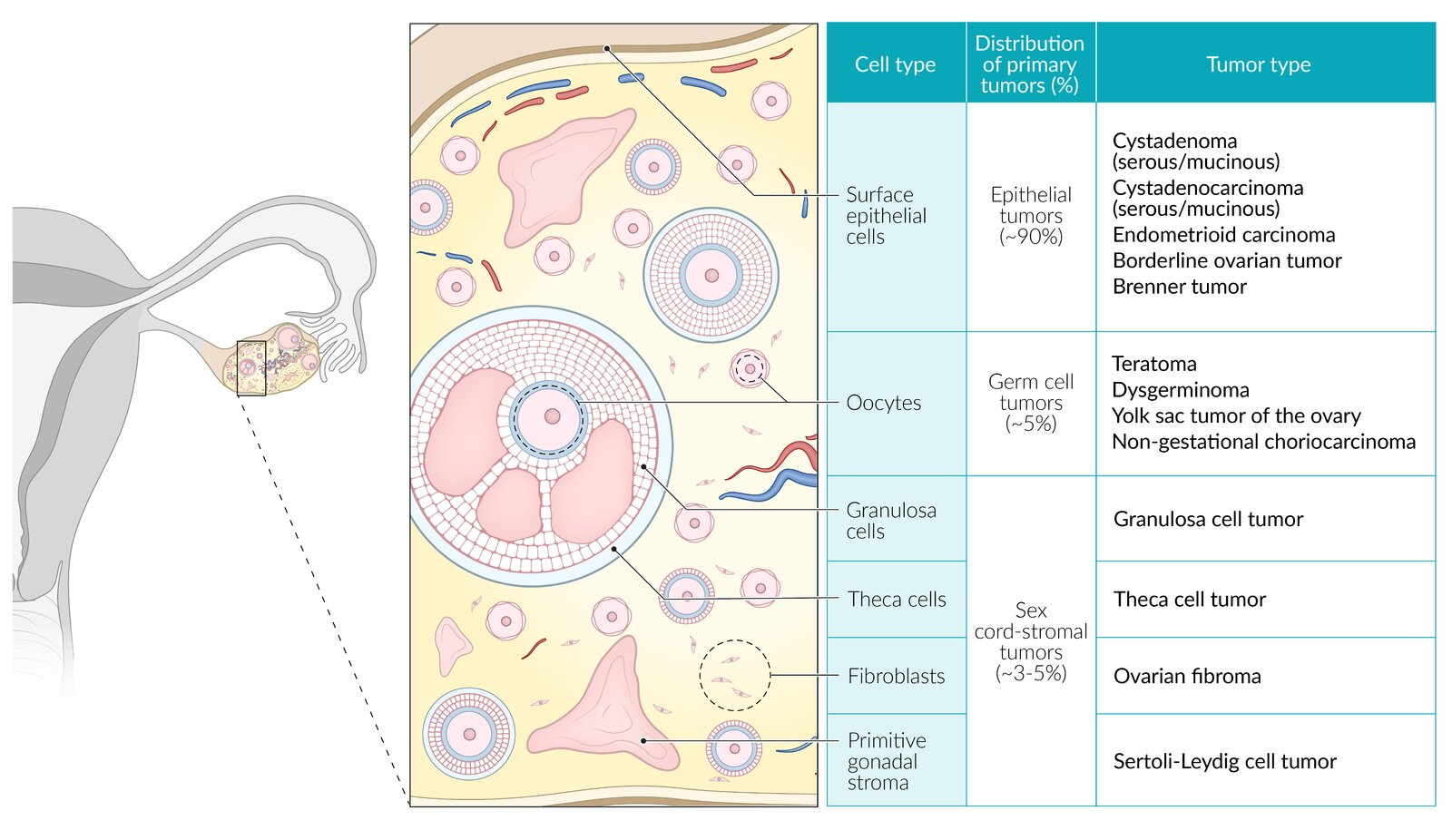
- Surface epithelial-stroma: composed of cells that support the normal ovarian structure for ovulation (eg, serous, mucinous epithelial cells).
- Germ cell: composed of cells that can develop into an embryo or placenta. These tumors are composed of varying amounts of germ layers (ie, endoderm, mesoderm, ectoderm), yolk sac, or placenta (eg, chorion). They often have associated hormonal activity (eg, increased hCG, alpha fetoprotein).
- Sex cord-stroma: composed of cells that support and surround the oocyte. These cells secrete sex hormones including estrogen (granulosa cells) and testosterone (Sertoli-Leydig cells).
| Histologic type | Diagnosis | Key features |
|---|---|---|
| Epithelial | Serous cystadenocarcinoma | Most common ovarian cancer Often bilateral Histology: psammoma bodies |
| Mucinous cystadenocarcinoma | Pseudomyxoma peritonei Mucin-producing epithelial cells |
|
| Germ cell | Dysgerminoma | Adolescents ↑ β-hCG, ↑ LDH Histology: "fried-egg" cells |
| Endodermal sinus (yolk sac) | ↑ AFP Aggressive Schiller-Duval bodies resembling glomeruli |
|
| Stroma (sex cord) | Granulosa cell tumor | ↑ Estrogen (e.g., endometrial hyperplasia, postmenopausal bleeding) ↑ Inhibin Histology: Call-Exner bodies, coffee-bean nuclei |
| Sertoli-Leydig cell tumor | ↑ Androgens (e.g., hirsutism, clitoromegaly) |
Ovarian germ cell tumors
Epithelial ovarian tumors
Cystadenoma
- Ovarian serous cystadenoma and Ovarian mucinous cystadenoma
- Most (serous) and second most common (mucinous) benign ovarian tumor
- Histology
- Ovarian serous cystadenoma
- May contain small papillary projections
- Psammoma bodies
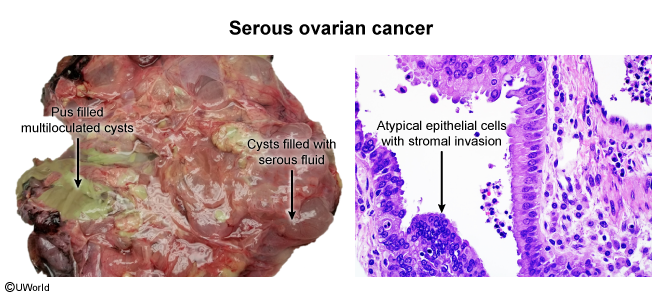
- Cyst is lined by serous epithelial cells (similar to the epithelium of fallopian tubes)
- Ovarian mucinous cystadenoma
- Cyst is lined by columnar epithelium that secretes thick mucus (similar to the epithelium of cervix)
- Ovarian serous cystadenoma
Ovarian germ cell tumors
- Subtypes are determined by structural differentiation
- Extraembryonic differentiation: yolk sac tumor
- Somatic differentiation: teratoma
- No differentiation: dysgerminoma
Diagnostics
Tumor markers
- Epithelial ovarian tumors: CA-125 is elevated in ∼ 80% of malignant tumors.
- Germ cell tumors
- Dysgerminoma: LDH, β-hCG
- Yolk sac tumor: AFP
- Immature teratoma: AFP, LDH, CA-125
- Choriocarcinoma: β-hCG
- Embryonal carcinoma: AFP, β-hCG
- Sex cord-stromal tumors:
- Granulosa cell tumor: inhibin