Epidemiology
- Prevalence: most common congenital gastrointestinal tract anomaly
- Rule of 2s for Meckel’s Diverticulum
- 2% of the population
- 2 feet from the ileocecal valve
- 2 inches in length
- 2 years old is the most common age for symptomatic presentation t
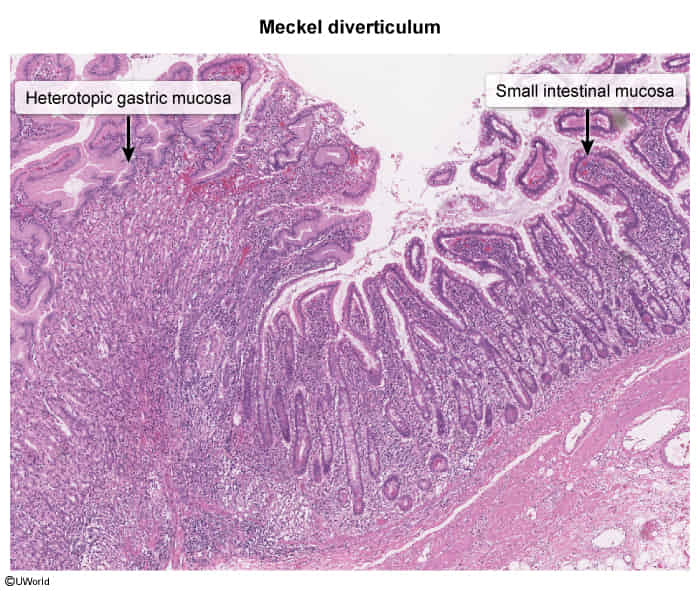
- 2 types of heterotopic mucosa (gastric and pancreatic)
Etiology
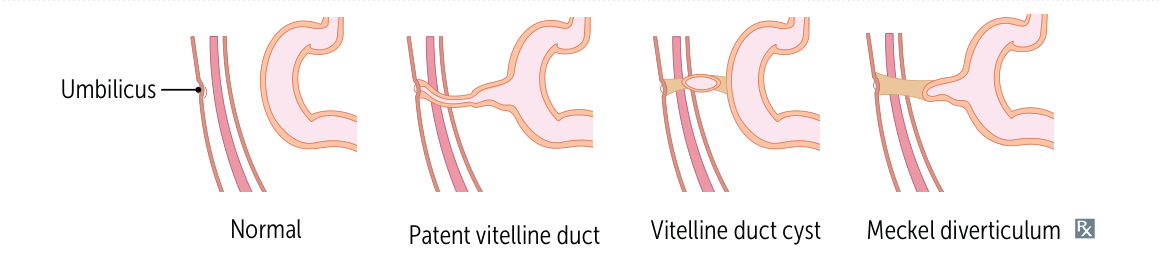
- True congenital diverticulum resulting from incomplete obliteration of the vitelline (omphalomesenteric) duct.
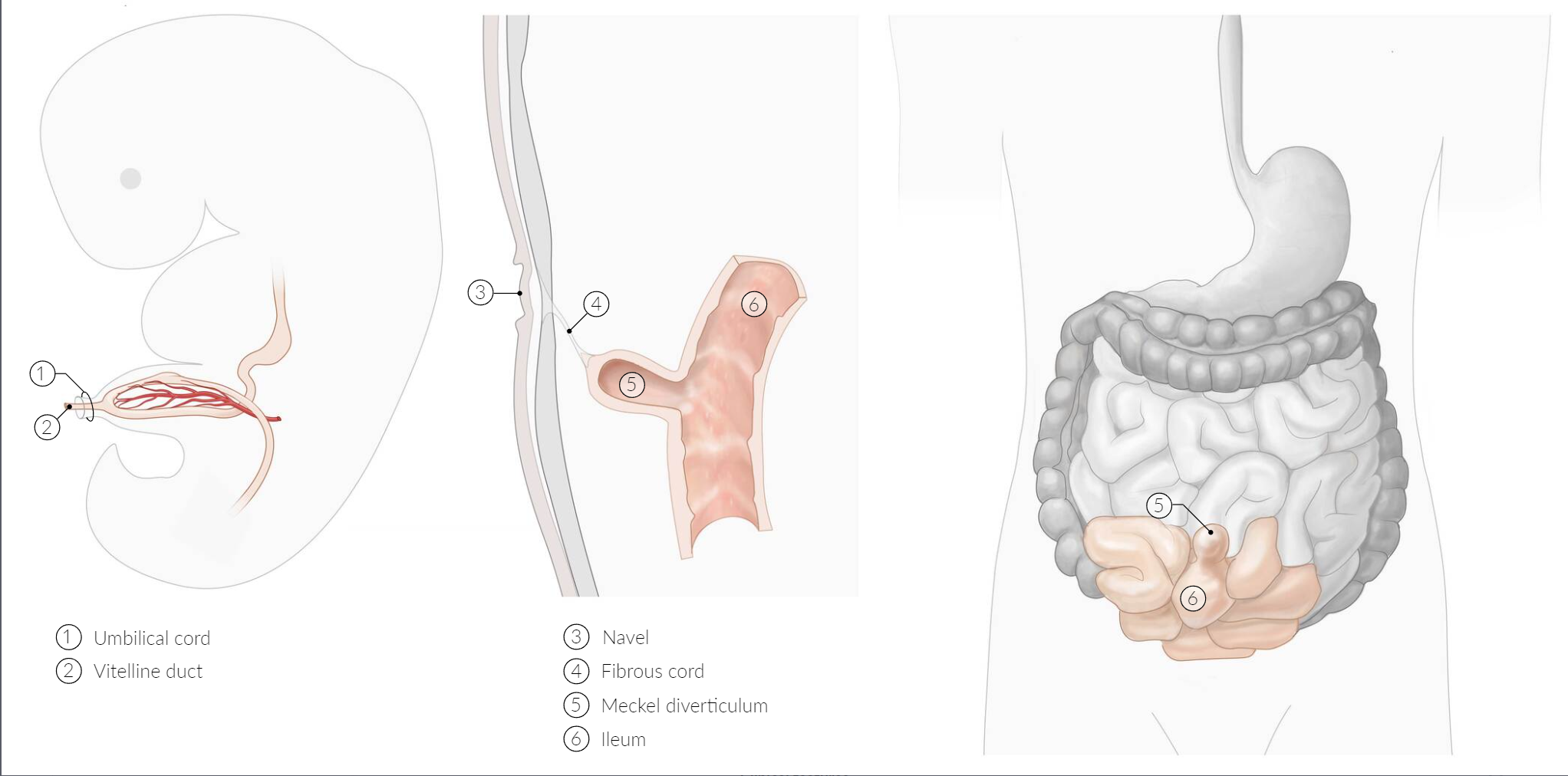
- Contains all three layers of the small intestine wall.
- Often contains ectopic tissue, most commonly gastric mucosa (>60%), which can secrete acid and cause ulceration and bleeding. Pancreatic tissue is the second most common.
- The vitelline duct is lined with pluripotent cells, meaning they have the ability to differentiate into various types of specialized cells.
- The vitelline duct is lined with pluripotent cells, meaning they have the ability to differentiate into various types of specialized cells.
Tip
Similar to Urachal abnormalities
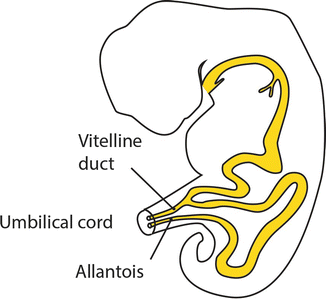
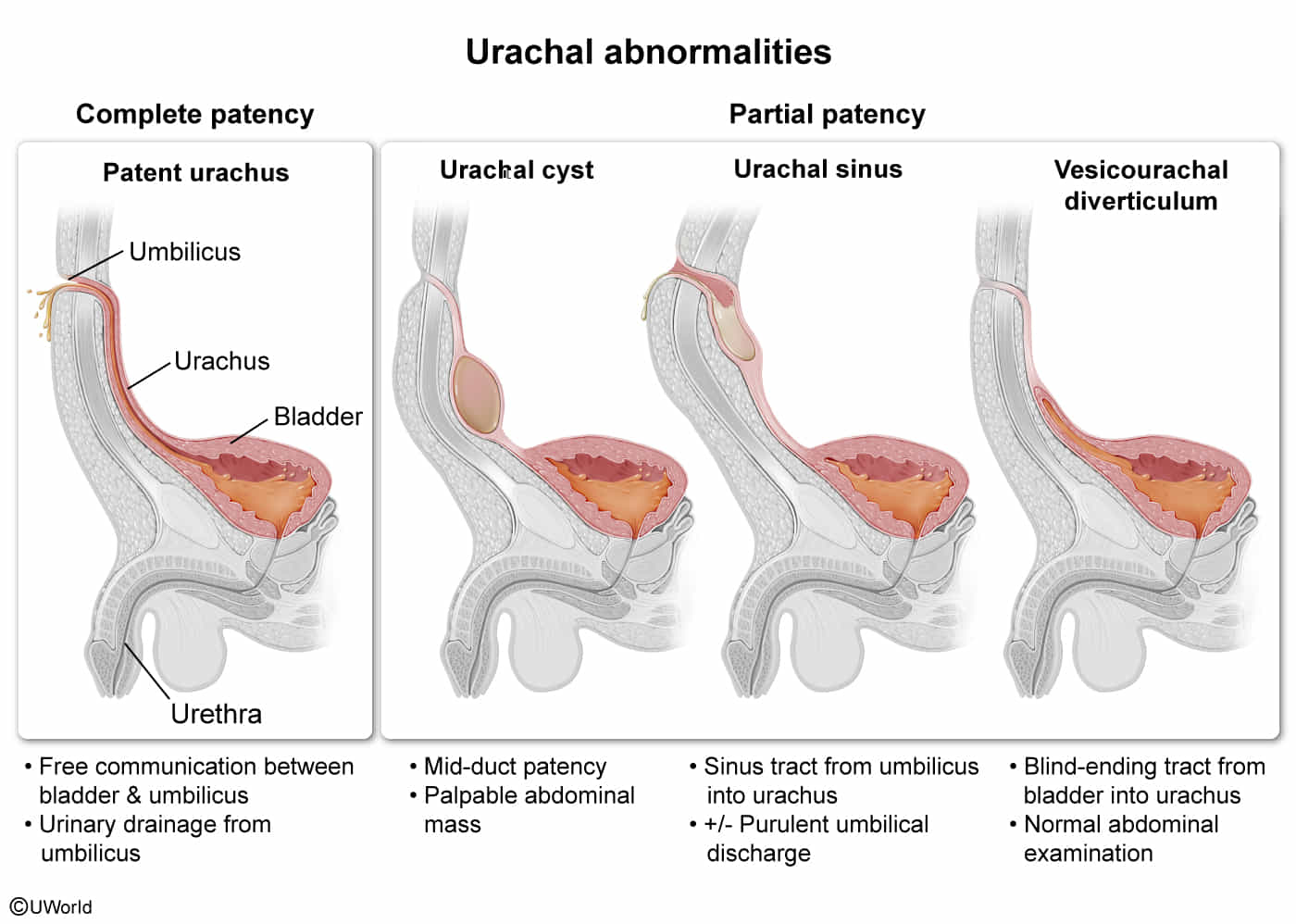
| Feature | Vitelline Duct | Allantois (Urachus) |
|---|---|---|
| Connects | Midgut to Yolk Sac | Bladder to Umbilicus |
| Adult Remnant | None (normally) | Median Umbilical Ligament |
| Pathology | Meckel Diverticulum | Patent Urachus |
| Classic Sx | Painless rectal bleeding (child) | Urine discharge from umbilicus |
| Cancer Risk | N/A | Adenocarcinoma of bladder (dome) |
Pathophysiology
Clinical features
- Most are asymptomatic and found incidentally.
- If symptomatic, classic presentation is painless rectal bleeding (maroon or “currant jelly” stools) in a child < 2 years old.
- Can also present with symptoms of complications like intestinal obstruction or diverticulitis (mimicking appendicitis).
- In adults, intestinal obstruction is the most common presentation, while bleeding is less frequent.
Diagnostics
Meckel scintigraphy scan (Meckel scan): a noninvasive nuclear medicine imaging technique using radiolabelled technetium (99mTc), which is preferentially absorbed by the gastric mucosa and can identify ectopic gastric mucosa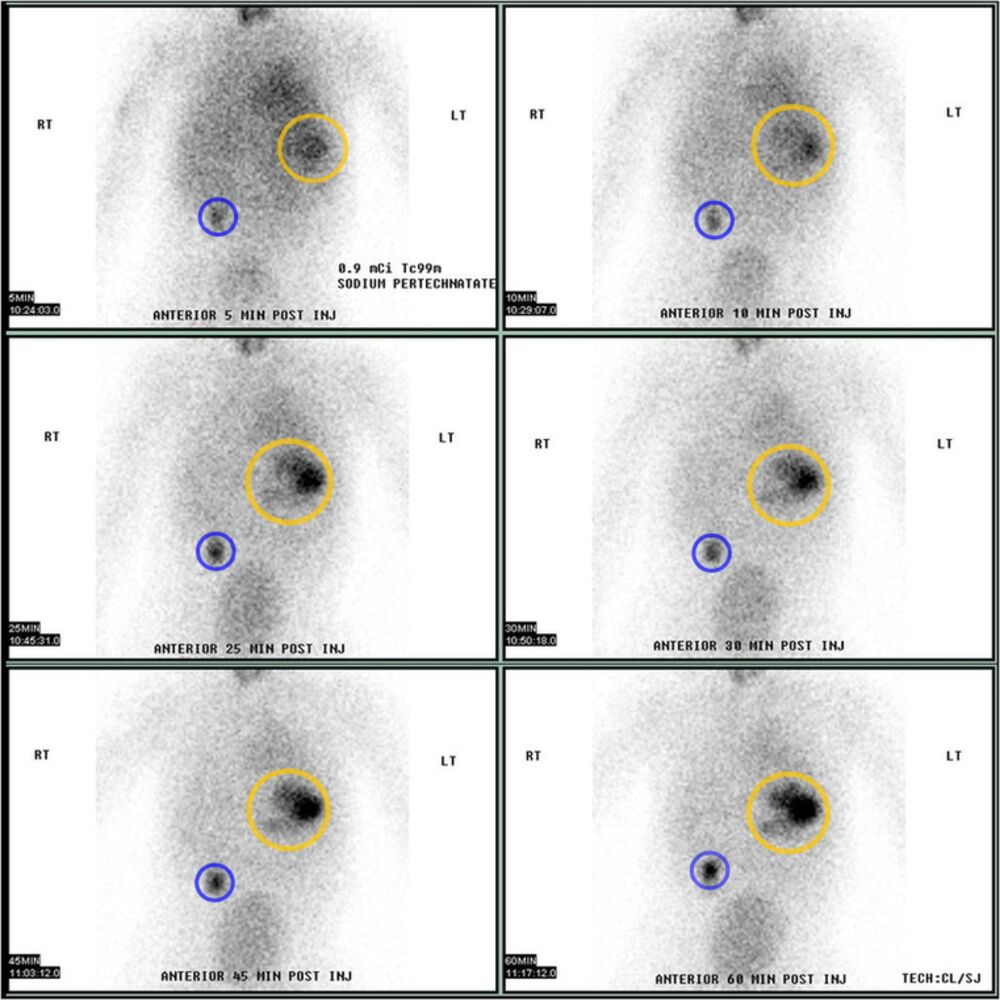
Treatment
Complications
- Bowel obstruction (usually affects terminal ileum) due to
- Intussusception
- Volvulus