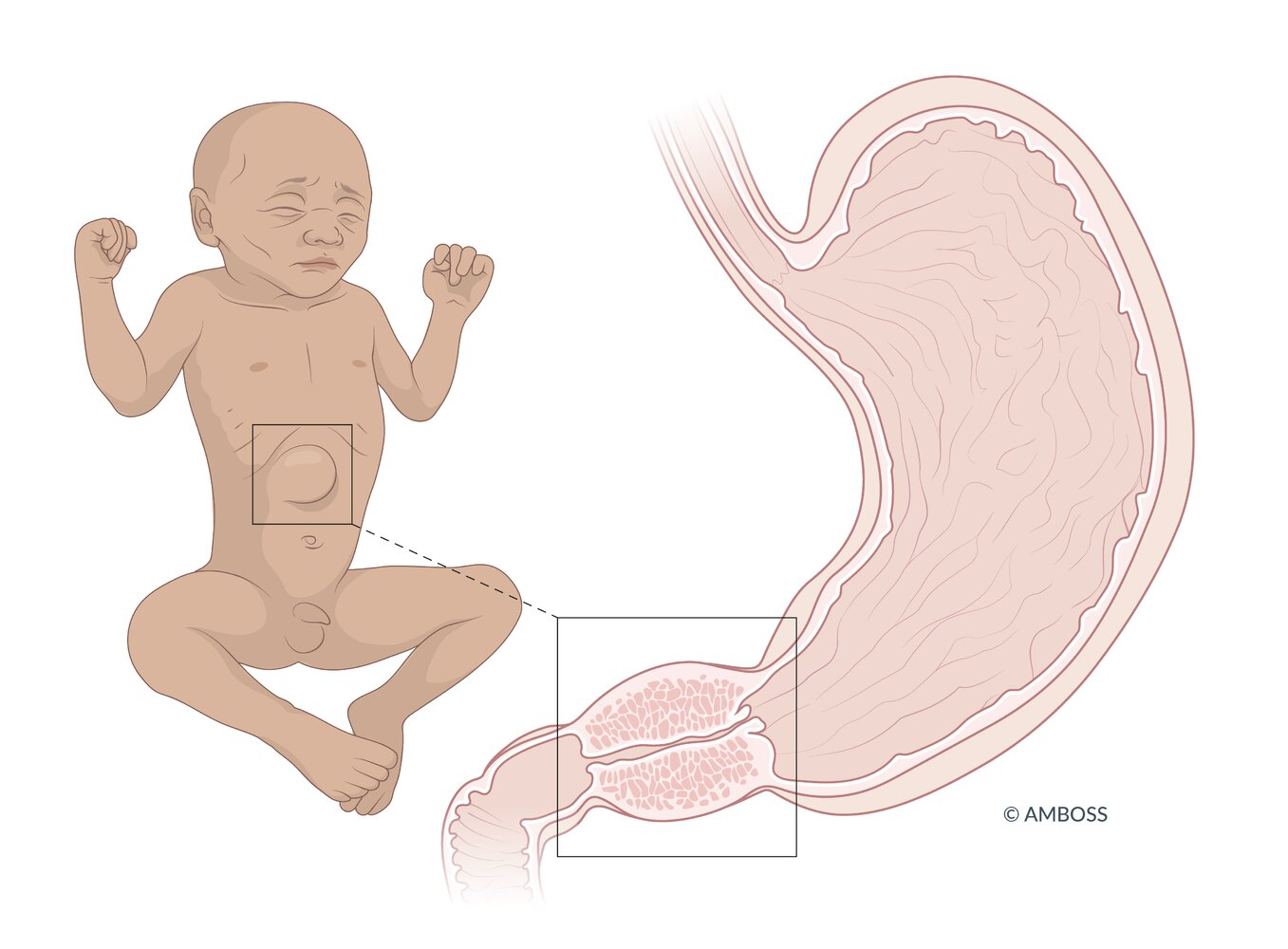
Hypertrophic pyloric stenosis is the most common cause of gastric outlet obstruction in infants.
Epidemiology
Etiology
- Environmental factors
- Exposure to nicotine during pregnancy
- Bottle feeding
- Bottle-fed infants drink more milk in less time, which may lead to pylorus muscle hypertrophy through overstimulation. Another hypothesis maintains that formula components make it harder to digest and gastric emptying is delayed, which may also burden the pylorus muscle.
- Macrolide antibiotics: Erythromycin and azithromycin are associated with an increased risk of hypertrophic pyloric stenosis, especially when administered within 2 weeks after birth.
Pathophysiology
- Hypertrophy and hyperplasia of the muscular layers of the pylorus (smooth muscle).
- Results in gastric outlet obstruction.
- Non-bilious vomiting causes loss of gastric HCl → Metabolic consequences.
Clinical features
- Onset: Typically 2–6 weeks of age.
- Non-bilious projectile vomiting immediately after feeding. t
- “Hungry vomiter”: Infant is hungry immediately after vomiting and wants to feed again.
- Physical Exam:
- Palpable “olive-shaped” mass in the epigastrium or RUQ.
- Visible peristaltic waves moving from left to right across the abdomen.
- Signs of dehydration (sunken fontanelle, ↓ skin turgor).
Diagnostics
- Hypochloremic hypokalemic metabolic alkalosis
- ± Indirect hyperbilirubinemia
- Commonly due to dehydration, which increases enterohepatic circulation of bilirubin.
- Ultrasound: thickened, elongated pylorus
Differential diagnostics
- Gastroesophageal Reflux (GER): “Happy spitter,” no metabolic alkalosis, usually non-projectile.
- Duodenal Atresia: Bilious vomiting, “Double bubble” sign on X-ray, associated with Down syndrome.
- Congenital Adrenal Hyperplasia (21-hydroxylase deficiency): Vomiting + virilization/salt-wasting (hyponatremia, hyperkalemia).