Hydatidiform mole
Tip
- Hydatidiform mole: need sperm + oocyte.
- Teratoma: just oocyte.
Epidemiology
Etiology
Tip
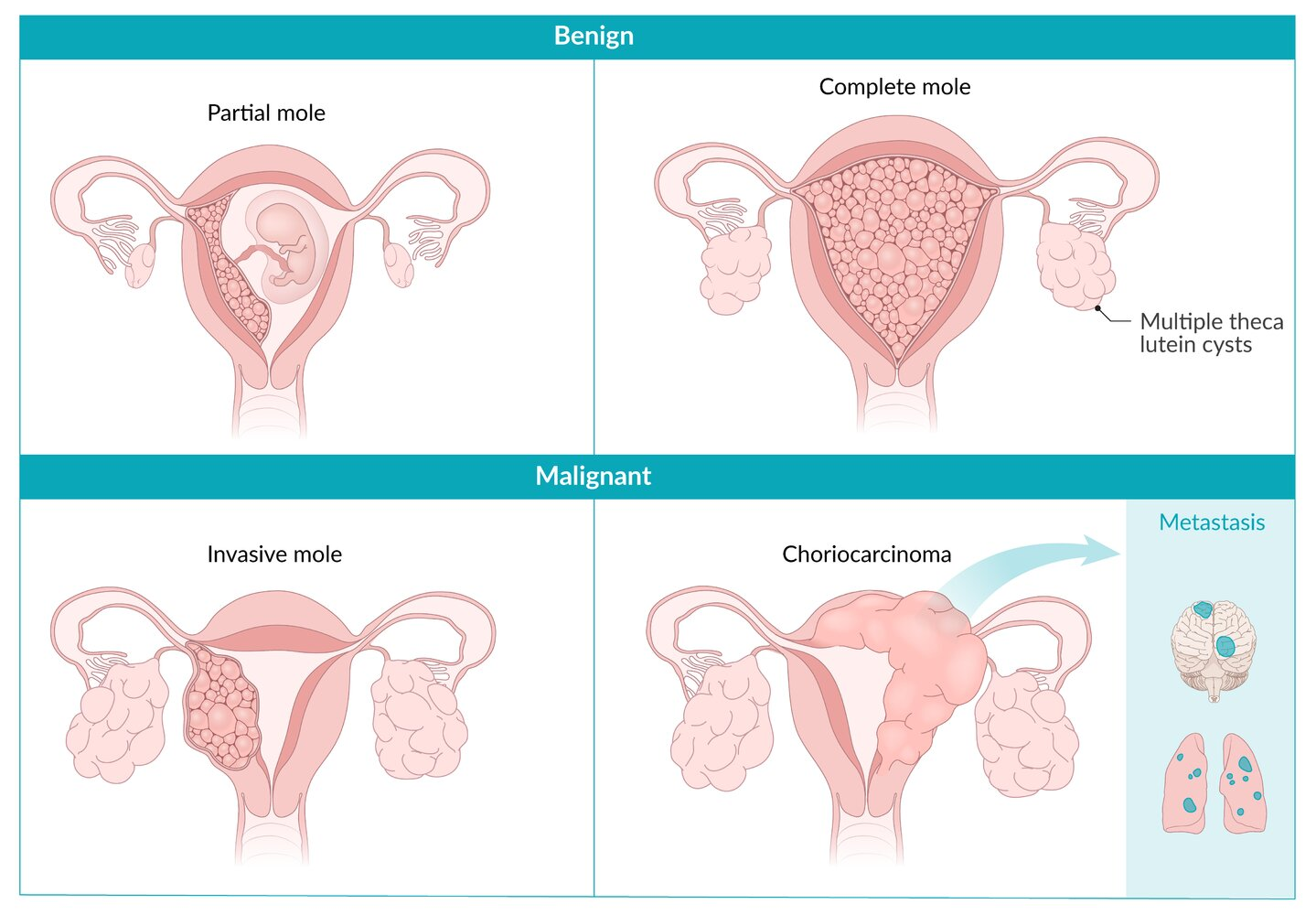
The terms "partial" and "complete" refer to the extent of abnormal tissue growth and the presence or absence of fetal tissue. In a complete mole, no normal tissue is present, whereas in a partial mole, there may be some but it’s still non-viable.
Complete mole
- Fertilization of an empty egg that does not carry any chromosomes by a single sperm
- The (physiological) haploid chromosome set contributed by the sperm is subsequently duplicated.
- Fetal karyotypes
- 46XX (more common; ∼ 90% of cases)
- 46XY (less common; ∼ 10% of cases)
Partial mole
- Fertilization of an egg containing a haploid set of chromosomes with two sperms
- Fetal karyotypes
- 69XXY
- 69XXX
Pathophysiology
Clinical features
- Vaginal bleeding during the first trimester
- Uterus size greater than normal for gestational age
- Pelvic pressure or pain
- Passage of vesicles with grape-like appearance
- β-hCG-mediated endocrine conditions
- Theca lutein cysts
- Preeclampsia (before the 20th week of gestation)
- Hyperemesis gravidarum
- Hyperthyroidism: Very high amounts of hCG may lead to hyperthyroidism because the α-subunit of hCG structurally resembles TSH.
Diagnostics
DDx