Usually occurs in pre-menopausal women, likely hormone mediated
Etiology
Pathophysiology
Benign, non-cancerous changes in breast tissue related to an exaggerated response to ovarian hormones (estrogen and progesterone). It is the most common breast lesion.
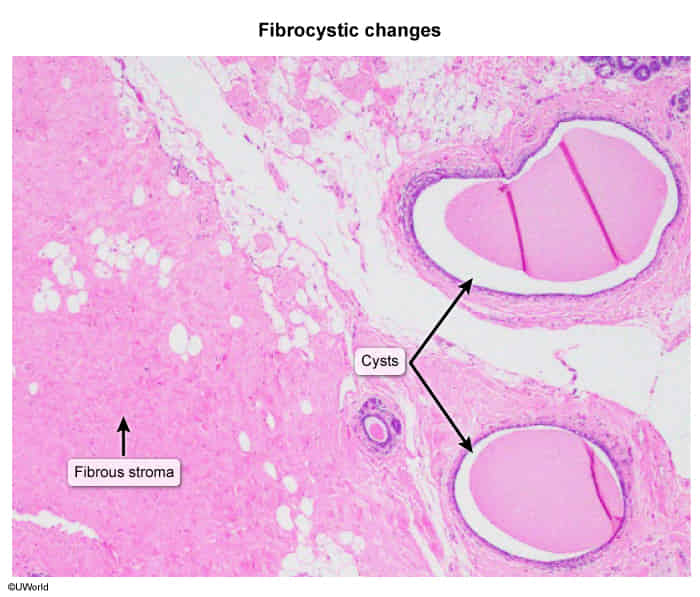
Characterized by a combination of fibrosis (thickening of stromal tissue), adenosis (proliferation of glandular tissue), and cyst formation.
Symptoms typically fluctuate with the menstrual cycle, worsening in the premenstrual (luteal) phase.
Clinical features
Demographics: Most common in premenopausal women, typically between ages 20 and 50. Symptoms usually subside after menopause unless a woman is on hormone replacement therapy.
Symptoms: Cyclical, bilateral breast pain (mastalgia) or tenderness, especially in the upper outer quadrants.
Physical Exam: Palpable lumps or “lumpiness” that may feel rubbery, rope-like, or nodular. Masses are often multiple, mobile, and may fluctuate in size with the menstrual cycle. A serous, non-bloody nipple discharge can occur.
Fibroadenoma: Typically a single, well-circumscribed, firm, rubbery, non-tender, and highly mobile mass. More common in younger women (<35).
Breast Cancer: Usually a single, hard, non-tender, immobile mass with irregular borders. May be associated with skin dimpling, nipple retraction, or bloody discharge.
Fat Necrosis: Often related to a history of breast trauma; may present as a firm, irregular mass, sometimes with skin retraction or calcifications on mammogram that can mimic cancer.
Mastitis: Presents with signs of infection like fever, erythema, and warmth, often in lactating women.