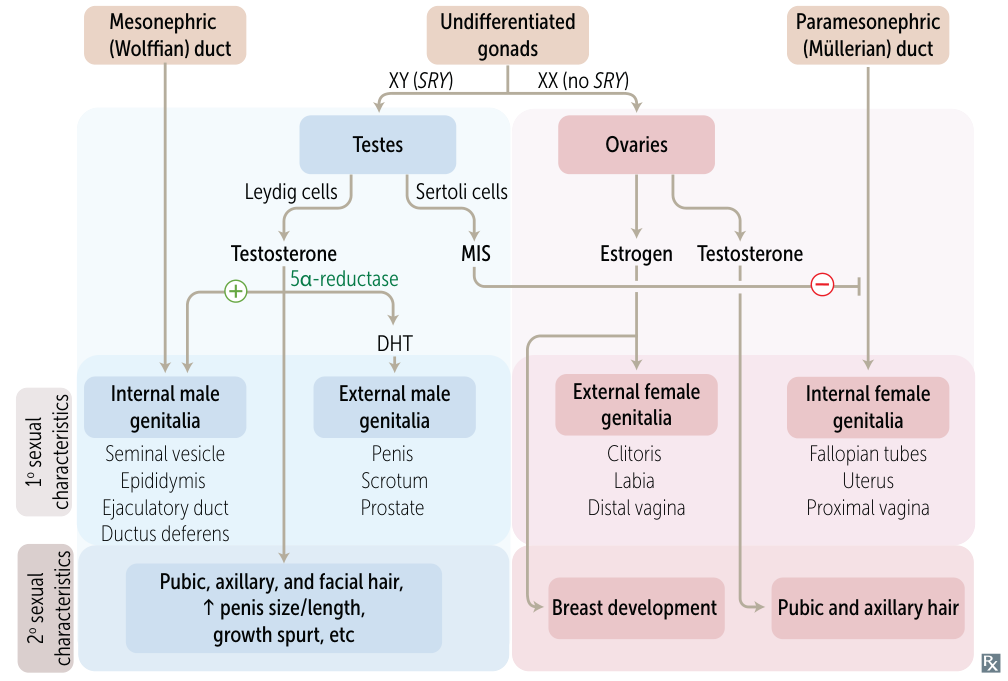
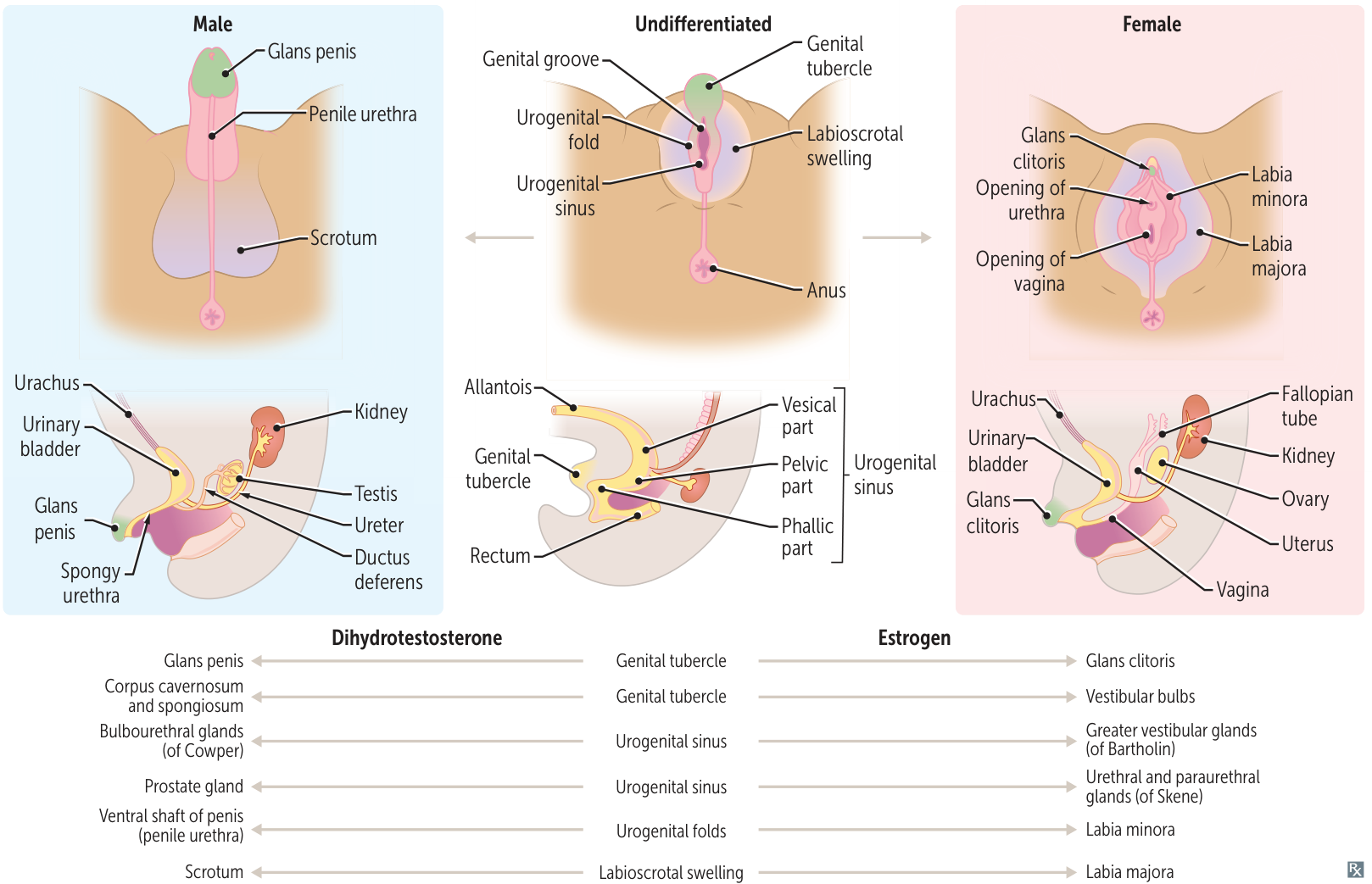
External Genitalia: Testosterone is converted to dihydrotestosterone (DHT) by 5α-reductase. DHT is responsible for the development of male external genitalia (penis, scrotum) and prostate.
3. Female Development
Key Driver:Absence of the SRY gene. Considered the “default” pathway.
Gonads: Primitive gonads develop into ovaries.
Ductal System:
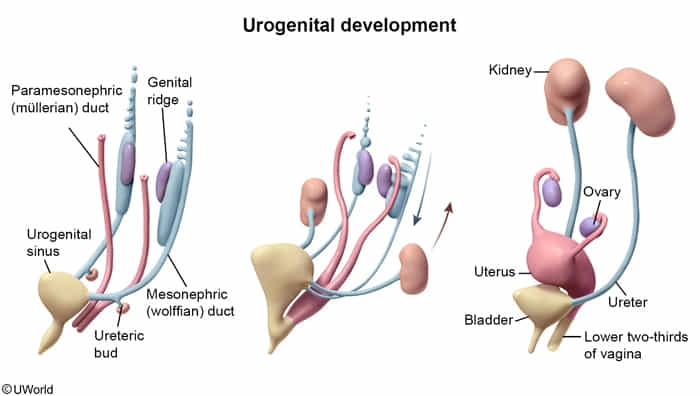
No MIS/AMH from Sertoli cells → Paramesonephric (Müllerian) ducts persist and develop into female internal structures: Fallopian tubes, uterus, cervix, and upper 1/3 of the vagina.
No testosterone from Leydig cells → Mesonephric (Wolffian) ducts degenerate.
External Genitalia: Develop in the absence of DHT. The genital tubercle becomes the clitoris, urethral folds become the labia minora, and labioscrotal swellings become the labia majora.
4. Summary of Homologous Structures
Indifferent Structure
Male Derivative (stimulated by Androgens)
Female Derivative (default)
Gonad
Testis
Ovary
Genital Tubercle
Glans penis, Corpus cavernosum/spongiosum
Glans clitoris, Vestibular bulbs
Urogenital Sinus
Bladder, Urethra, Prostate, Bulbourethral glands
Bladder, Urethra, Lower 2/3 of vagina, Bartholin glands