Urinary incontinence
Epidemiology
- Stress incontinence and mixed incontinence are the most common types of incontinence in female patients.
- Urge incontinence is the most common type in male patients.
Etiology
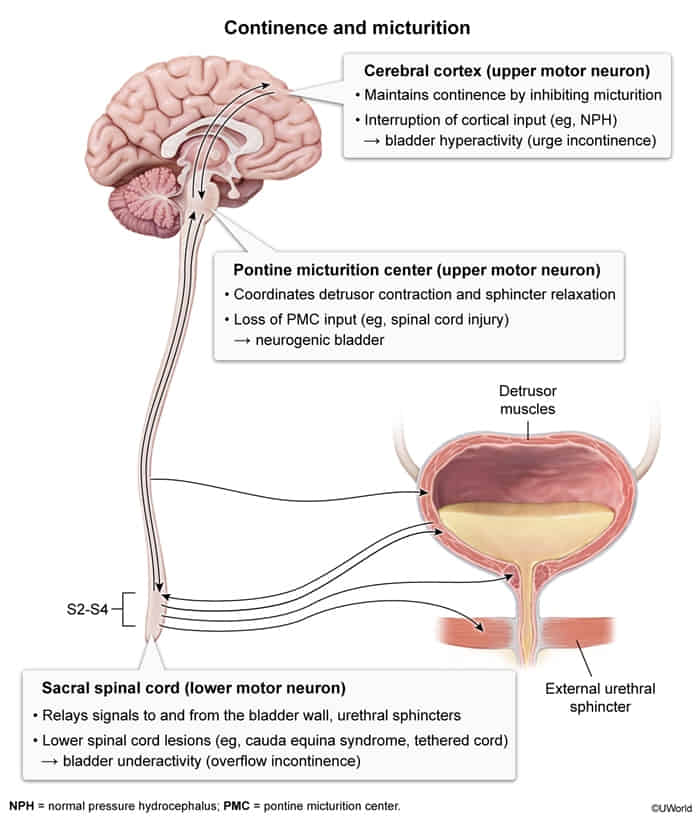
- Neurological causes
- Multiple sclerosis
- Spinal injury
- Normal pressure hydrocephalus
- Genitourinary causes
- Trauma to the pelvic floor
- Intrinsic sphincter deficiency
- Urethral hypermobility in women
- Impaired detrusor contractility
- Bladder outlet obstruction
- Pelvic floor weakness
- Transient causes of urinary incontinence
- Drugs (e.g., diuretics)
- Urinary tract infections
- Postmenopausal atrophic urethritis
- Psychiatric causes (especially depression, delirium/confused state)
- Excessive urinary output (in conditions like hyperglycemia, hypercalcemia, CHF)
- Stool impaction
- General risk factors
- Recurrent urinary tract infections
To remember the reversible causes of acute urinary incontinence, think DIAPPERS: Delirium/confusion, Infection, Atrophic urethritis/vaginitis, Pharmaceutical, Psychiatric causes (especially depression), Excessive urinary output (hyperglycemia, hypercalcemia, CHF), Restricted mobility, Stool impaction.
Classifications
Overflow incontinence
Mechanism
- Impaired (weak) detrusor contractility
- Bladder outlet obstruction (e.g., BPH)
- Both mechanisms can lead to incomplete bladder emptying → bladder overfilling → chronically distended bladder with ↑ bladder pressure → dribbling of urine (leak) when intravesical pressure > outlet resistance
Clinical features
- Frequent, involuntary intermittent/continuous dribbling of urine in the absence of an urge to urinate
- Occurs only when the bladder is full
- Postvoid residual urine volume (seen on ultrasound or with catherization)
- Assess for urinary retention via bladder scan (≥200 mL) or straight catheterization yielding ≥200 mL urine output.
Treatment
- Intermittent catheterization: for scheduled bladder emptying
- Intermittent -> prevention of catheter-associated UTIs and is favored by most patients; indwelling catheters may be considered if necessary.
Neurogenic bladder dysfunction
Mechanism
detrusor sphincter dyssynergia
- Simultaneous contractions of the detrusor muscle and involuntary activation of the urethral sphincter → blockage of bladder outlet → small amounts of urine are pressed through the contracted sphincter muscle → high intravesical pressure along with inappropriate contraction of the urethral sphincter
- Commonly seen in multiple sclerosis and spinal cord injury
Clinical features
- Voiding and/or storage dysfunction, intermittent voiding, urinary retention
- Irregular, small volume incontinence without an associated urge to void (sometimes referred to as reflex incontinence)
Total incontinence
Complete loss of sphincter function (due to previous surgery, nerve damage, metastasis) → Urinary leakage occurs at all times
Clinical features
Diagnostics
Treatment
Overview of pharmacotherapy


The use of muscarinic agonists may lead to urinary urgency, while the use of sympathomimetics or muscarinic antagonists may lead to urinary retention, especially if there is an untreated outlet obstruction.
No pharmacological therapies are FDA-approved for stress incontinence; treatment is primarily conservative with surgery.