- Anatomical Classification
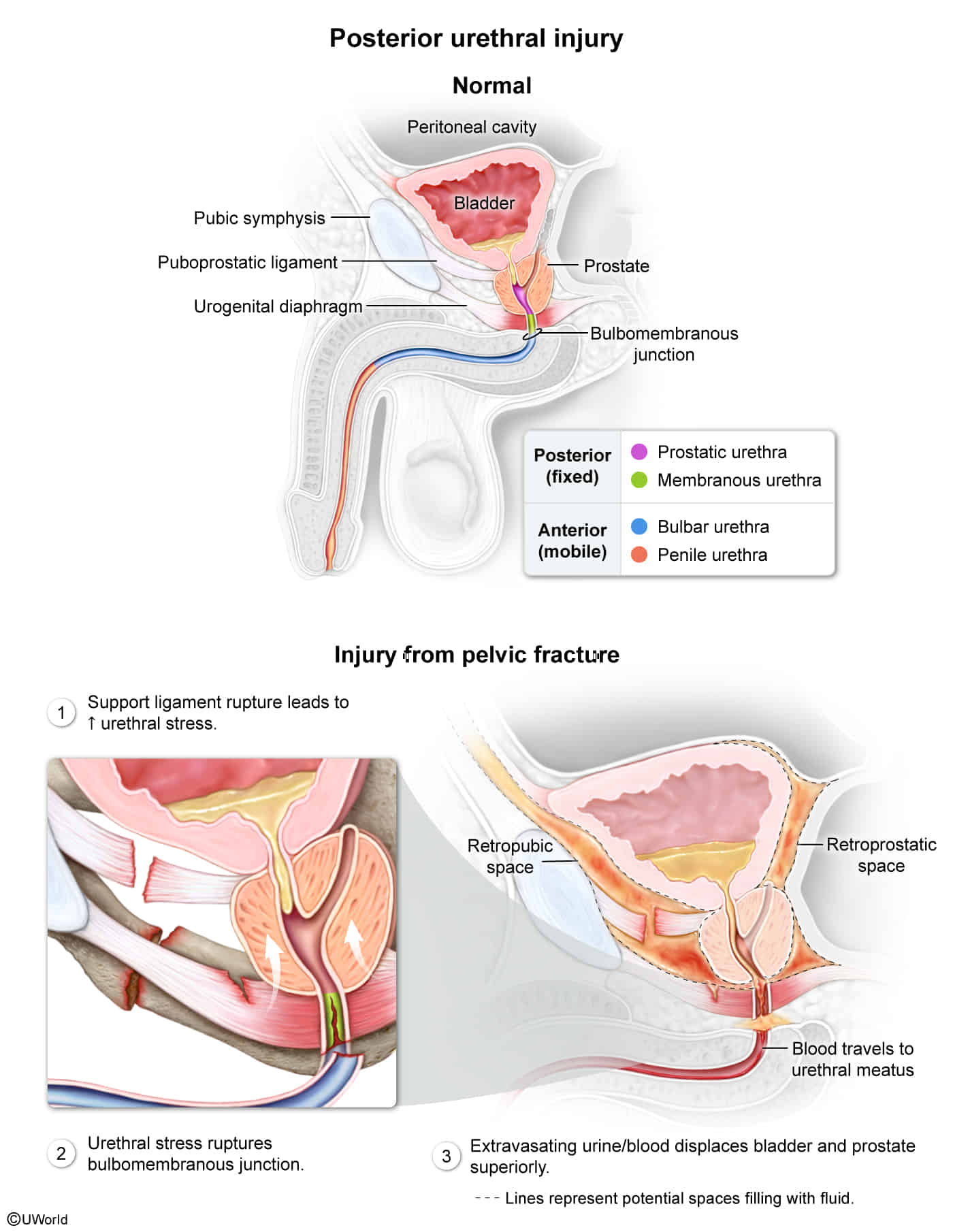
- Posterior Urethra: Membranous (narrowest, most common site of injury) and Prostatic segments.
- Anterior Urethra (Spongy urethra): Bulbar and Penile segments. t
- Etiology
- Posterior Urethral Injury:
- Associated with pelvic fractures (e.g., MVA).
- Shearing force at the prostatomembranous junction.
- Anterior Urethral Injury:
- Associated with straddle injuries (e.g., falling on a bicycle crossbar), direct perineal trauma, or instrumentation t .
- Crushing of the bulbar urethra against the pubic symphysis.
- Clinical Presentation
- Triad: Blood at urethral meatus, urinary retention, bladder distention.
- Posterior Specific:
- High-riding prostate on digital rectal exam (DRE) due to hematoma/disruption of puboprostatic ligaments.
- Scrotal hematoma may be present but less prominent than anterior.
- Anterior Specific:
- Perineal hematoma (butterfly pattern if Buck’s fascia is intact; extensive tracking if Buck’s fascia is ruptured).
- Diagnostics
- Retrograde Urethrogram (RUG): First step to rule out injury. Shows dye extravasation.
- Management
- Contraindication: NO Foley catheter insertion (blind passage creates false tract).
- Acute Tx: Suprapubic catheter (cystostomy).
- Definitive: Surgical repair.