- Etiology/Pathophysiology
- Decreased Intake
- Alcohol use disorder (multifactorial: poor intake, renal wasting, diarrhea).
- Malnutrition.
- Total parenteral nutrition (TPN) with insufficient Mg2+.
- GI Losses
- Diarrhea: Chronic diarrhea from any cause (e.g., IBD, celiac disease).
- Malabsorption syndromes (e.g., celiac disease, Crohn’s disease, short bowel syndrome).
- Medications: Proton pump inhibitors (PPIs) (chronic use), laxatives.
- Renal Losses
- Diuretics: Loop and thiazide diuretics are a major cause.
- Alcohol: Directly causes renal magnesium wasting.
- Uncontrolled diabetes (osmotic diuresis).
- Nephrotoxic drugs: Amphotericin B, cisplatin, aminoglycosides, cyclosporine.
- Inherited tubular disorders: Gitelman syndrome, Bartter syndrome.
- Redistribution
- Refeeding syndrome.
- Treatment of diabetic ketoacidosis (DKA).
- Decreased Intake
- Clinical Features
- Neuromuscular:
- Hyperexcitability: Tremors, muscle cramps, fasciculations.
- Tetany: Positive Chvostek sign (facial muscle twitch) and Trousseau sign (carpopedal spasm).
- Seizures, lethargy, weakness.
- Cardiovascular:
- Arrhythmias: Torsades de pointes (polymorphic ventricular tachycardia), premature ventricular contractions (PVCs), atrial fibrillation.
- EKG findings: Prolonged QT interval, prolonged PR interval, widened QRS.
- Associated Electrolyte Abnormalities:
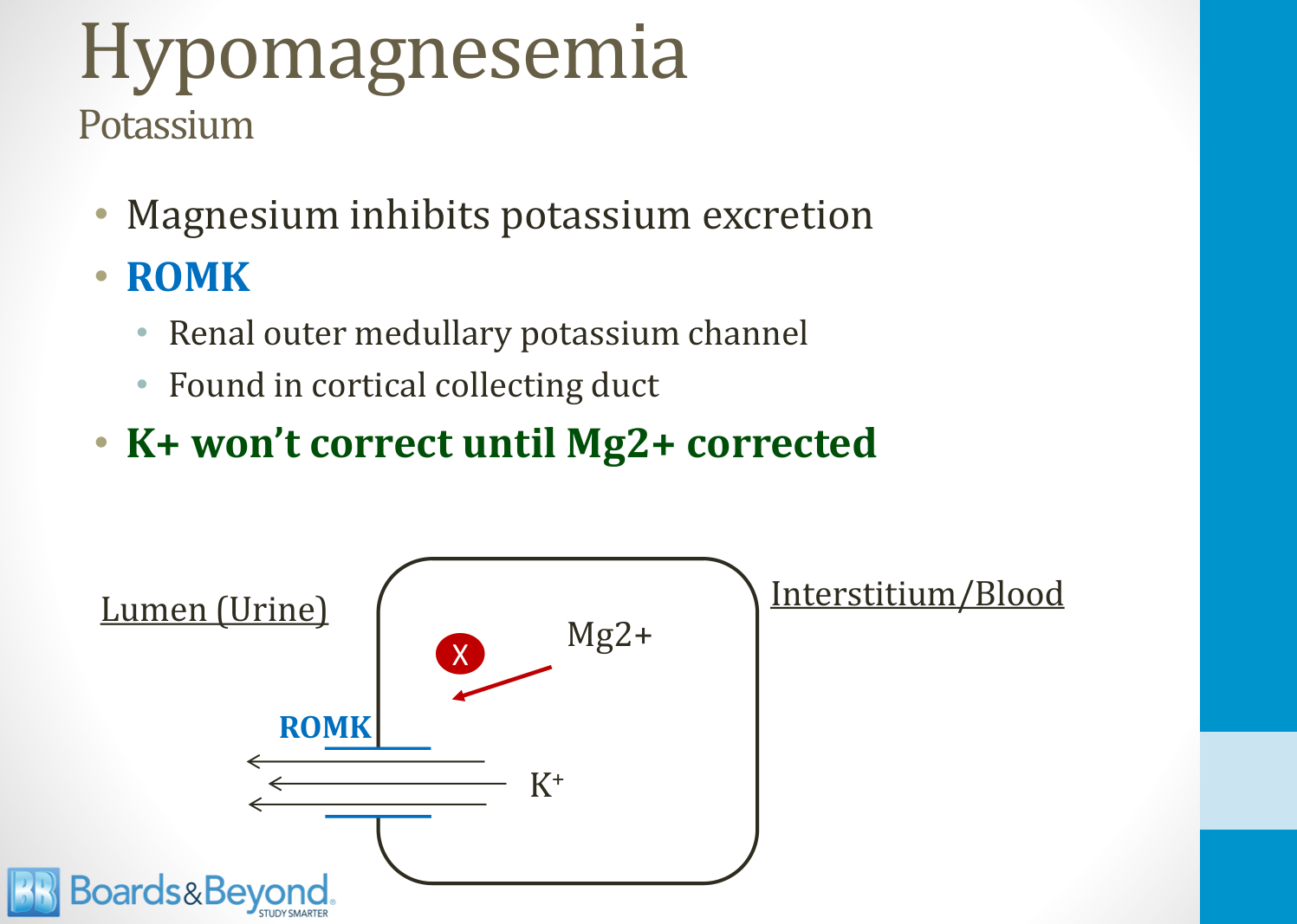
- Refractory Hypokalemia: Mg2+ is a cofactor for ROMK channels in the kidney, which excrete K+. Low Mg2+ leads to increased K+ wasting. Hypokalemia will not correct without Mg2+ repletion.
- Hypocalcemia: Low Mg2+ impairs PTH secretion and causes end-organ resistance to PTH.
- Neuromuscular:
- Diagnostics
- Serum Mg2+ level < 1.8 mg/dL (< 0.7 mmol/L).
- Check other electrolytes, especially K+ and Ca2+, which are often concurrently low.
- EKG to evaluate for arrhythmias and QT prolongation.
- To differentiate renal vs. GI losses:
- Fractional excretion of magnesium (FEMg):
- <2% suggests GI/inadequate intake (kidneys are conserving Mg2+).
-
2% suggests renal wasting.
- Fractional excretion of magnesium (FEMg):
- Treatment
- Asymptomatic/Mild:
- Oral magnesium oxide.
- Symptomatic/Severe (e.g., arrhythmias, seizures, Torsades):
- IV magnesium sulfate (MgSO₄).
- Always correct Mg2+ before or concurrently with K⁺ in patients with refractory hypokalemia.
- Asymptomatic/Mild:
Clinical features
- Neuromuscular excitability
- Tetany, tremor
- Cardiac arrhythmias
- Hypocalcemia
- Hypokalemia