Core Concepts
- Definition: An experimental study design where participants are randomly assigned to an experimental group (receives intervention) or a control group (receives placebo or standard of care).
- “Gold Standard”: Considered the highest level of evidence for determining the efficacy and causality of a therapeutic or preventive intervention.
- Objective: To minimize bias when testing the effectiveness and safety of a new intervention.
Key Features
- Randomization:
- Each participant has an equal chance of being assigned to any group.
- Purpose: To minimize selection bias and control for confounding variables (both known and unknown) by distributing them evenly among the groups.
- Allocation Concealment: The process of hiding the next allocated group from the person enrolling the participant, which prevents selection bias during recruitment.
- Control Group:
- The group that receives a placebo, no treatment, or the current standard of care.
- Purpose: Provides a baseline to compare the effect of the new intervention against.
- Blinding (Masking):
- Concealing group allocation from individuals involved in the trial to prevent bias.
- Single-blind: Only the participant is unaware of their assigned group.
- Double-blind: Both the participant and the investigators/clinicians are unaware of the group assignments. This is the most common and preferred method.
- Triple-blind: Participants, investigators, and data analysts are all unaware of group assignments.
- Purpose: Reduces performance bias (systematic differences in care) and ascertainment/observer bias (distorted outcome assessment).
Trial Designs & Phases
- Common Designs:
- Parallel Group: Each group receives a different treatment simultaneously (most common design).
- Crossover: Each participant receives both treatments in a sequence, separated by a “washout” period. Participants serve as their own controls.
- Factorial: Tests two or more interventions simultaneously using various combinations.
Clinical trials
Mnemonic
Does the drug SWIM?
“Is it Safe?” Assesses safety, toxicity, pharmacokinetics, and pharmacodynamics
- Phase 0 trial
- Purpose: Exploratory phase with no therapeutic or diagnostic intent, aimed at gaining insight into pharmacokinetics and pharmacodynamics.
- Only < 1% of the therapeutic dose is used.
- Safety and toxicity are not assessed.
- Study population: Small sample consisting of either healthy individuals or a population with a disease of interest (∼ 10–15).
- Study design: Open-label.
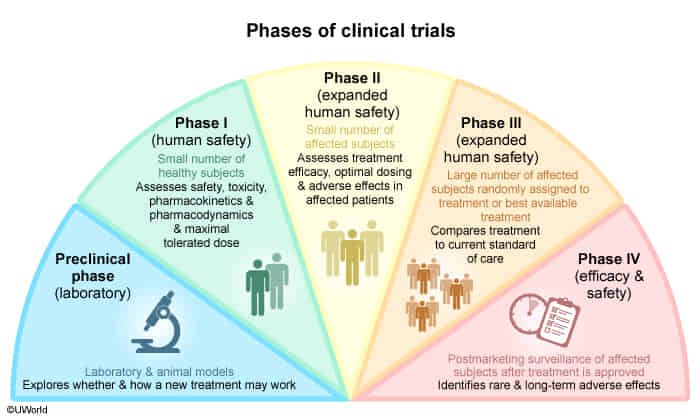
- Phase I trial
- Purpose: Evaluation of pharmacodynamic and pharmacokinetic properties of the drug, safety, and toxicity.
- Evaluation of the maximum tolerated dose.
- Study population: Small number of healthy individuals or patients with a specific disease (∼ 15–30).
- Study design: Open-label.
- Phase II trial
- Purpose: Evaluation of efficacy, optimal dose range, and side effects (especially common and short-term side effects).
- Study population: Moderate number of patients with a specific disease (∼ 10–100).
- Study design: Randomized, Controlled, Anonymized.
- Phase III trial
- Purpose: Final confirmation of safety and evaluation of efficacy against placebo or the current standard of care.
- Study population: Randomized control trial with a large number of patients with a specific disease (∼ 100–1000).
- Study design: Randomized Controlled Trial.
- Phase IV trial
- Purpose: Postmarketing surveillance, comparing real-life efficacy to that described in research studies. Safety studies following approval (especially evaluation of rare and long-term side effects).
- Study population: Large number of patients with a specific disease after drug approval.
- Study design: Open-label.
Analysis & Interpretation
- Intention-to-Treat (ITT) Analysis:
- All participants are analyzed in the groups to which they were originally randomized, regardless of whether they completed or adhered to the treatment protocol.
- Benefit: Preserves the benefits of randomization and gives a more realistic measure of the treatment’s effectiveness in a real-world setting. Minimizes bias from attrition.
- Per-Protocol Analysis:
- Only includes participants who strictly adhered to the protocol.
- Risk: Breaks randomization and is more susceptible to bias, but may provide a better measure of the treatment’s effect under ideal conditions.
Potential Biases & Limitations
- Selection Bias: Systematic differences between groups at baseline. Minimized by randomization and allocation concealment.
- Performance Bias: Systematic differences in the care provided to groups (apart from the intervention). Minimized by blinding.
- Detection/Ascertainment Bias: Systematic differences in how outcomes are assessed. Minimized by blinding of outcome assessors.
- Attrition Bias: Systematic differences in withdrawals or loss to follow-up between groups. Addressed by Intention-to-Treat analysis.
- Limitations of RCTs:
- Costly and time-consuming.
- Ethical concerns (e.g., withholding treatment, lack of clinical equipoise).
- Limited external validity (generalizability): Strict inclusion/exclusion criteria may result in a study population that is not representative of the general patient population.