Epidemiology
- Peak incidence: 60–70 years
Classification
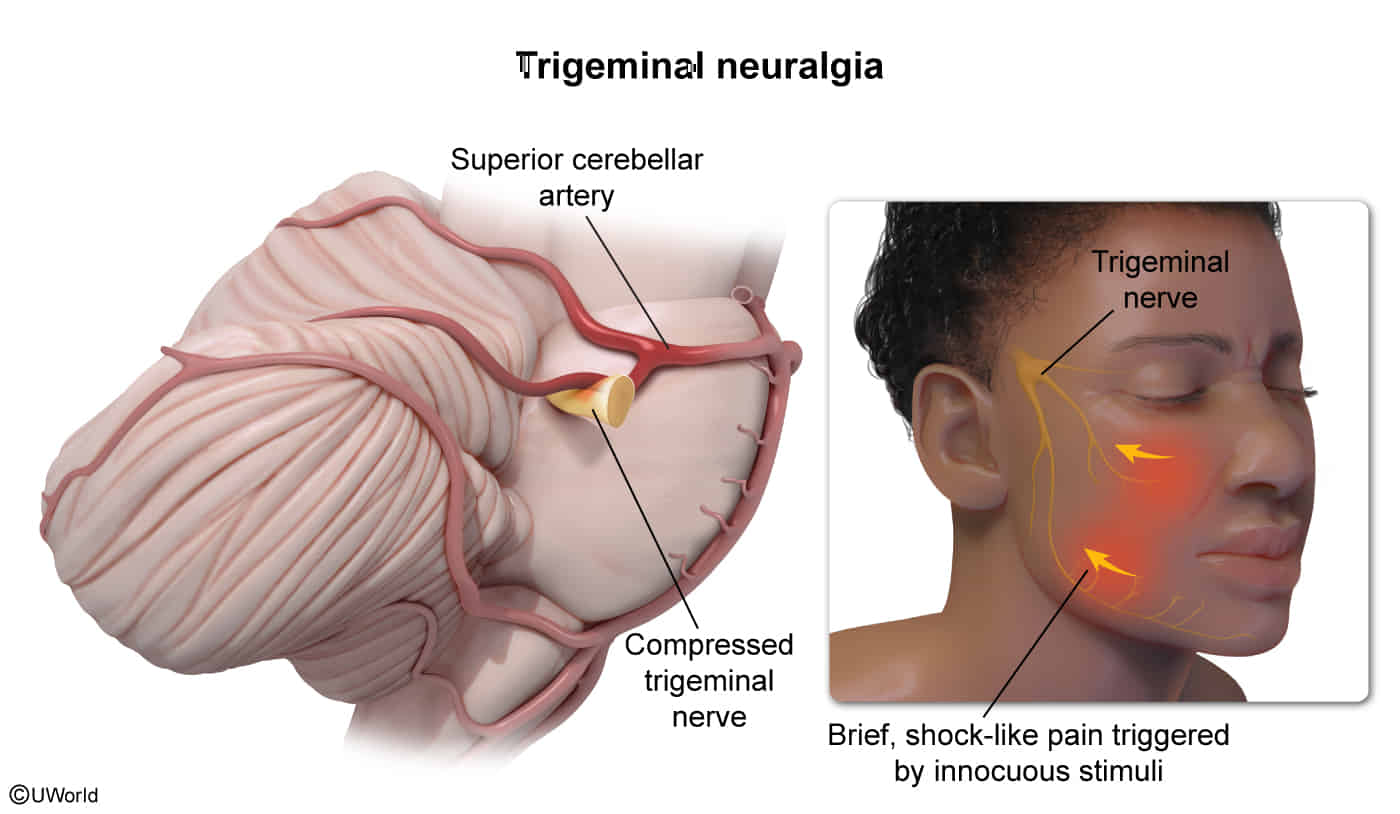
- Most common cause is neurovascular compression of the trigeminal nerve root (CN V) by a superior cerebellar artery loop.
- Pulsatile compression by an artery strips the myelin off the trigeminal nerve root.
- This loss of insulation creates a “short-circuit” (ephaptic transmission).
- Now, normal touch signals (carried by A-beta fibers) cross-activate adjacent pain fibers (A-delta/C fibers).
- This is why innocuous stimuli (e.g., touch) trigger maximal pain. The sudden, electric shock quality is due to spontaneous, high-frequency firing from the unstable, demyelinated nerve.
- Other causes (secondary trigeminal neuralgia): Multiple sclerosis (MS), tumors (e.g., acoustic neuroma), AVMs. Suspect in younger pts or with bilateral Sx.

Clinical features
- Unilateral facial pain: paroxysmal, severe shooting or stabbing (like an electric shock), followed by a burning ache
- Lasts several seconds (in rare cases, several minutes) and may occur up to 100 times per day
- Typically shoots from mouth to the angle of the jaw on the affected side
- Occurs either at rest or is triggered by movements such as chewing, talking, or touch (e.g., brushing teeth, washing face); becomes worse with stimulation
Diagnostics
Treatment
<% tp.file.cursor() %>