Aura Phase: Caused by Cortical Spreading Depression (CSD), a self-propagating wave of neuronal depolarization across the cortex (~3-5 mm/min). This initial hyperactivity is followed by suppression, explaining the positive (e.g., scintillating scotoma) and negative (e.g., scotoma) features of aura.
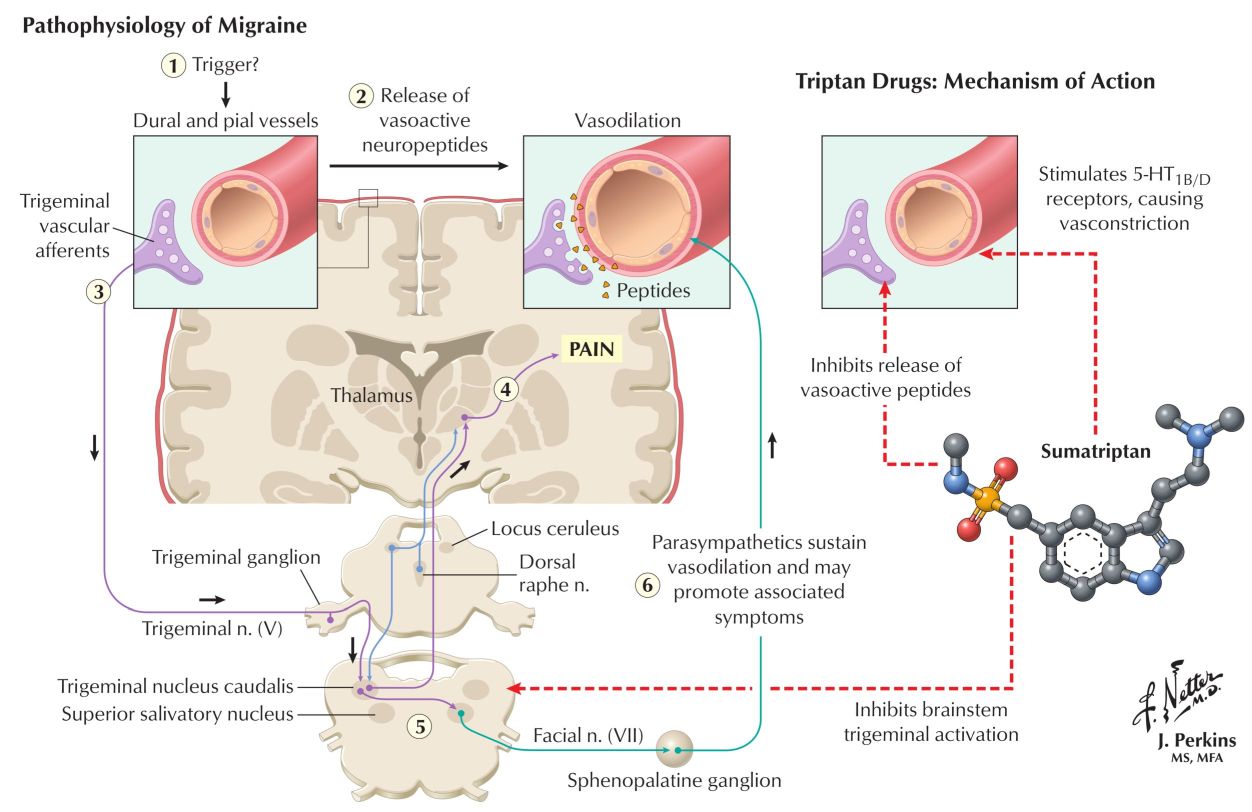
Pain Phase: Caused by activation of the Trigeminovascular System (TVS).
CSD is believed to trigger the activation of trigeminal nerve afferents that innervate cranial blood vessels.
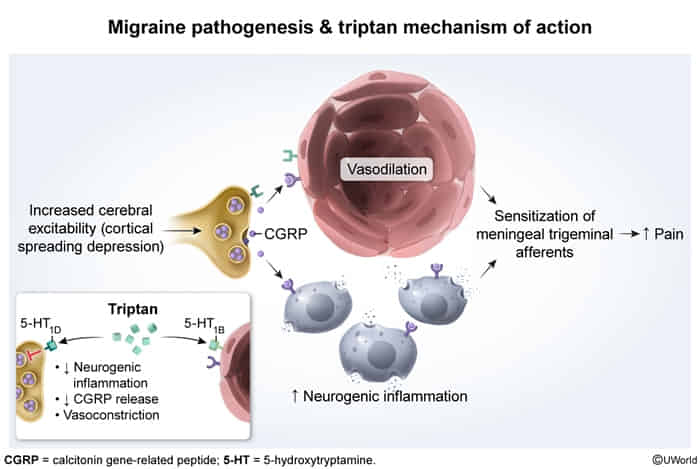
This activation causes the release of vasoactive neuropeptides, most importantly Calcitonin Gene-Related Peptide (CGRP).
Role of CGRP:
CGRP is a potent vasodilator and promotes neurogenic inflammation. This leads to sensitization of pain receptors on the meningeal vessels, causing the characteristic severe, throbbing headache.
CGRP levels are elevated during migraine attacks and normalize after successful treatment.
Pharmacologic Targets:Triptans inhibit CGRP release, while newer CGRP antagonists directly block the peptide or its receptor.
Clinical features
POUND Mnemonic:
Pulsatile/throbbing quality.
One-day duration (typically lasts 4–72 hours if untreated).
Unilateral location.
Nausea and/or vomiting.
Disabling intensity (moderate to severe), aggravated by routine physical activity.
Associated with photophobia (sensitivity to light) and phonophobia (sensitivity to sound).
Phases: Can include a prodrome (fatigue, mood changes), aura, headache, and postdrome (feeling drained).
Aura:Occurs in ~30% of patients. Usually transient (<60 mins) focal neurologic symptoms (e.g., scintillating scotoma, paresthesias) that precede or accompany the headache.