↑ ICP → ↓ CPP → compensatory activation of the sympathetic nervous system → ↑ systolic blood pressure → stimulation of aortic arch baroreceptors → activation of the parasympathetic nervous system (vagus) → bradycardia
↑ Pressure on brainstem → dysfunction of respiratory center → irregular breathing
Clinical features
Global
Cushing triad: irregular breathing, widening pulse pressure, and bradycardia
Increase in systolic, decrease in diastolic blood pressure
Reduced levels of consciousness
Headache
Vomiting
Papilledema
Psychiatric changes
In infants: macrocephaly, bulging fontanel, sunset sign
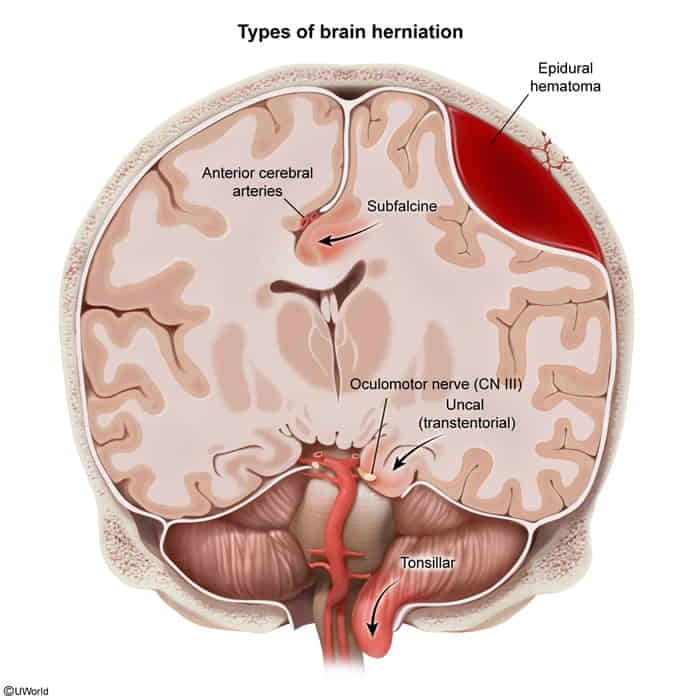
What: Cingulate gyrus is displaced under the falx cerebri. This is the most common type of herniation.
Vessels: Compression of the anterior cerebral artery (ACA) can occur.
Clinical signs: May be asymptomatic or cause contralateral lower limb weakness due to motor cortex ischemia.
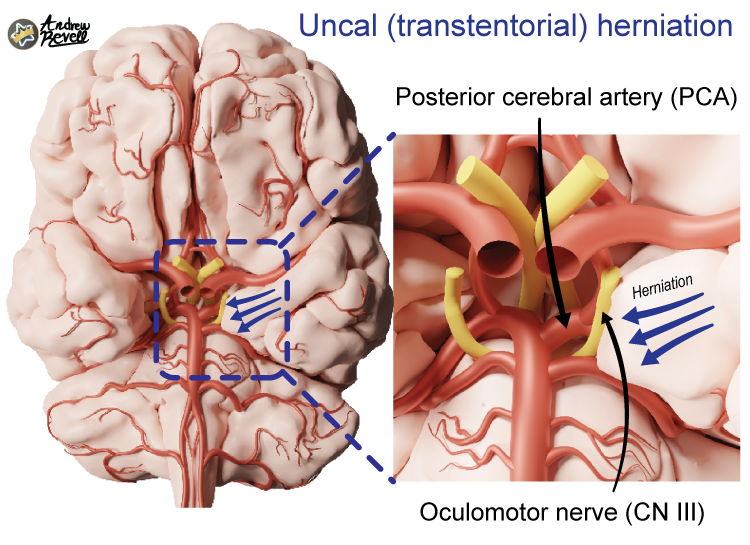
Transtentorial (Uncal)
What: Medial temporal lobe (specifically the uncus) is forced through the tentorial notch.
CN III Palsy: This is a classic and critical finding.
Early: Compression of parasympathetic fibers on the exterior of CN III causes an ipsilateral fixed and dilated pupil (“blown pupil”).
Late: Compression of motor fibers of CN III leads to a “down and out” gaze.
Vessels: Ipsilateral posterior cerebral artery (PCA) compression can cause contralateral homonymous hemianopsia.
Motor: Compression of the contralateral cerebral peduncle against the tentorium (Kernohan’s Notch) causes ipsilateral hemiparesis (a false-localizing sign).
Brainstem: Brainstem displacement can cause tearing of paramedian basilar artery branches, leading to fatal Duret hemorrhages.
Central Herniation
What: Downward displacement of the diencephalon and brainstem through the tentorial notch.
Clinical signs: Leads to a rapid decline in consciousness, decorticate posturing progressing to decerebrate posturing, and eventually death.
Tonsillar
What: Cerebellar tonsils are forced through the foramen magnum.
Clinical signs: Compresses the medulla, which contains the cardiorespiratory centers. This leads to respiratory arrest, circulatory collapse, and rapid death.
Clinical pearl: This is why a lumbar puncture (LP) is contraindicated in patients with suspected ↑ICP until an intracranial mass lesion has been ruled out by imaging (e.g., CT scan). An LP can create a pressure gradient that precipitates tonsillar herniation.