Scarlet fever
Epidemiology
Etiology
- Pathogen
- Group A β‑hemolytic streptococci (Streptococcus pyogenes) produce erythrogenic exotoxin A, B, or C
- These exotoxins cause the rash of scarlet fever via a delayed-type skin reaction.
- Group A β‑hemolytic streptococci (Streptococcus pyogenes) produce erythrogenic exotoxin A, B, or C
- Route of transmission: aerosol
Pathophysiology
Clinical features
Exanthem phase
- Rash manifests 12–48 hours after fever onset.
- Fine, erythematous, sandpaper‑like texture
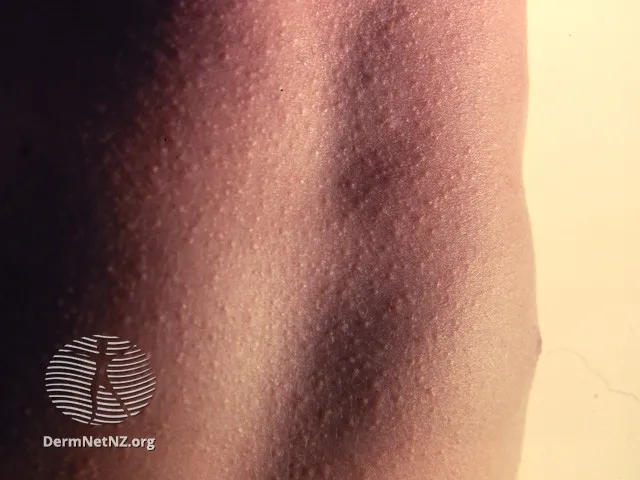
- Blanches with pressure, but nonblanching petechiae may also be present
- Begins on neck or trunk and spreads rapidly across the body (except for the palms and soles)
- Characteristic features include:
- Flushed cheeks with perioral pallor
- Strawberry tongue: bright red tongue color with papillary hyperplasia, which may initially be covered with a white coating
- Pastia lines
- A characteristic sign of scarlet fever
- Linear, petechial appearance
- Most pronounced in the groin, underarm, and elbow creases (i.e., flexural areas)
Diagnostics
| Feature | Scarlet Fever | Acute Rheumatic Fever |
|---|---|---|
| Timing | Concurrent with active GAS infection | Delayed (2–4 weeks post-infection) |
| Pathophysiology | Toxin-mediated (SPEs) | Immune-mediated (molecular mimicry) |
| Rash | "Sandpaper" texture, diffuse, punctate | Erythema marginatum (serpiginous, clear centers) |
| Key Finding | Strawberry tongue, Pastia's lines | Migratory polyarthritis, carditis, chorea |
| Treatment Goal | Eradicate active infection, prevent ARF | Reduce inflammation, prevent recurrence with long-term prophylaxis |
Treatment
- Initiate one of the recommended antibiotic regimens for acute GAS pharyngitis, e.g.:
- Oral penicillin V or amoxicillin
- Nonsevere penicillin reaction: oral cephalosporins (e.g., cephalexin)
- Severe penicillin reaction: oral macrolides (e.g., azithromycin) or clindamycin