Epidemiology
Etiology
- Common in adolescents and young adults (ages 10–35).
- Etiology unclear, but likely viral reactivation (HHV-6 and HHV-7).
- Often occurs in spring and autumn.
Pathophysiology
Clinical features
- Herald Patch:
- The initial lesion in ~80% of cases.
- Herald/mother = followed days later by other scaly erythematous plaques
- Single, large (2–10 cm), oval, salmon-colored plaque with a collarette of scale (inward-facing scale) at the border.
- Typically on the trunk.

- Secondary Eruption:
- Appears days to weeks after the herald patch.
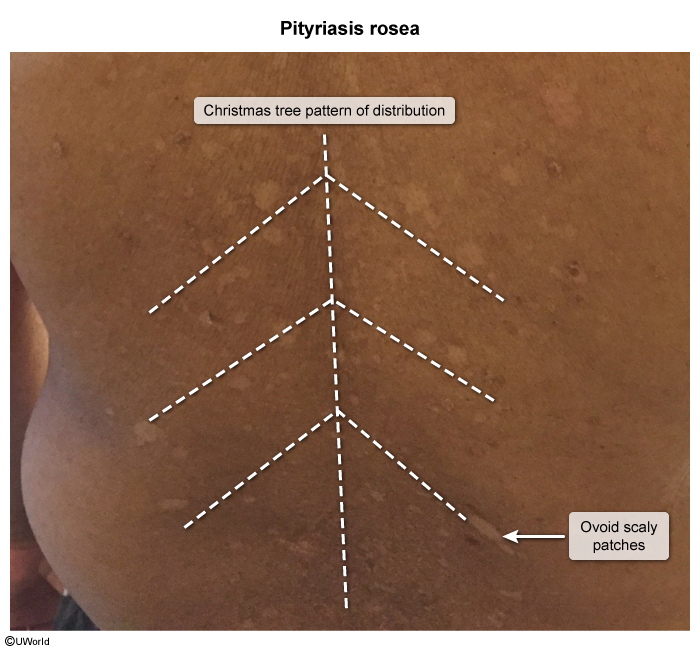
- Multiple smaller, scaly, oval plaques on the trunk and proximal extremities.
- “Christmas tree” distribution: Lesions follow the skin tension lines (Langer lines) on the back.
- Symptoms:
- Pruritus (itching) is variable (mild to severe).
- Prodrome (fever, malaise) is rare.
Diagnostics
- Primarily a clinical diagnosis.
- KOH preparation: Negative (rules out tinea corporis).
- RPR/VDRL: Negative (rules out secondary syphilis).
Differential Diagnosis
- Secondary Syphilis: Look for involvement of palms and soles (rare in PR) and history of chancre.
- Tinea Corporis: Scaly ring with central clearing; KOH positive.
- Guttate Psoriasis: Teardrop-shaped plaques, often follows Strep pharyngitis.
- Nummular Eczema: Coin-shaped, very itchy lesions
Treatment
- Self-limited: Spontaneously resolves in 6–8 weeks.