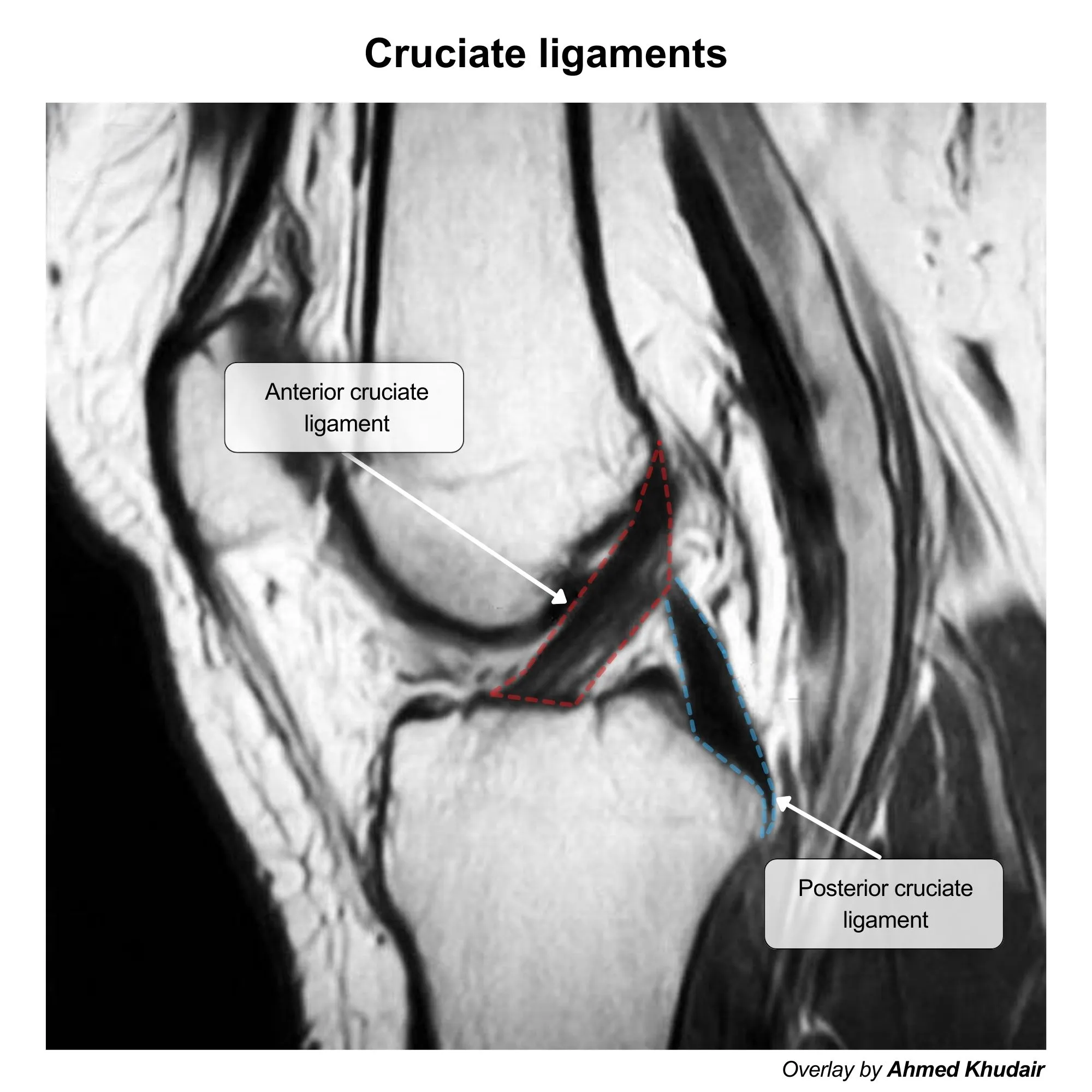
Cruciate ligament injuries
Lateral femoral condyle to anterior tibia: ACL. Medial femoral condyle to posterior tibia: PCL. LAMP.
Anterior Cruciate Ligament (ACL) Injury
- Function
- Primarily prevents anterior translation of the tibia relative to the femur.
- Provides rotational stability to the knee, resisting internal tibial rotation.
- Mechanism of Injury
- Most common knee ligament injury.
- Typically non-contact pivoting or twisting motion with the foot planted (e.g., soccer, basketball, skiing).
- Sudden deceleration or hyperextension.
- Clinical Presentation
- Pt often reports hearing or feeling a distinct “pop”.
- Rapid development of hemarthrosis (joint swelling due to bleeding) within hours.
- Sensation of instability or the knee “giving way.”
- Physical Examination
- Lachman Test: Most sensitive test. With knee flexed at 30°, stabilize femur and pull tibia anteriorly. Positive if excessive anterior translation without a firm endpoint.
- Anterior Drawer Test: With knee flexed at 90°, pull tibia anteriorly. (Less sensitive due to hamstring guarding).
- Pivot Shift Test: High specificity; reproduces the instability event.
- Associations
- “Unhappy Triad” (O’Donoghue’s Triad): Result of severe lateral force to the knee. Classically involves damage to the:
- ACL
- MCL (Medial Collateral Ligament)
- Medial Meniscus (Note: Modern literature suggests lateral meniscus is more commonly injured acutely, but USMLE traditionally emphasizes the medial meniscus).
- “Unhappy Triad” (O’Donoghue’s Triad): Result of severe lateral force to the knee. Classically involves damage to the:
- Diagnosis & Treatment
- MRI: Gold standard for confirmation.
- Tx: RICE, Physical Therapy. Surgical reconstruction (autograft/allograft) indicated for young, active patients or those with persistent instability.
Posterior Cruciate Ligament (PCL) Injury
- Function
- Primarily prevents posterior translation of the tibia relative to the femur.
- Strongest ligament in the knee; acts as a central axis of rotation.
- Mechanism of Injury
- Much less common than ACL injuries.
- “Dashboard Injury”: Direct posterior force applied to the proximal tibia with the knee flexed (e.g., knee hitting dashboard in MVA (motor vehicle accident)).
- Severe hyperflexion or hyperextension.
- Clinical Presentation
- Vague posterior knee pain.
- Instability (though often less pronounced than ACL).
- Swelling is typically mild to moderate compared to ACL.
- Physical Examination
- Posterior Drawer Test: With knee flexed at 90°, push tibia posteriorly. Positive if excessive posterior translation (tibia “sags” back).
- Posterior Sag Sign: With patient supine and hips/knees flexed to 90°, look for posterior subluxation of the tibia due to gravity.
- Diagnosis & Treatment
- MRI: Gold standard.
- Tx: Usually non-operative (bracing, intense quadriceps strengthening) for isolated Grade I/II injuries. Surgery reserved for multi-ligament knee injuries or failed conservative management.