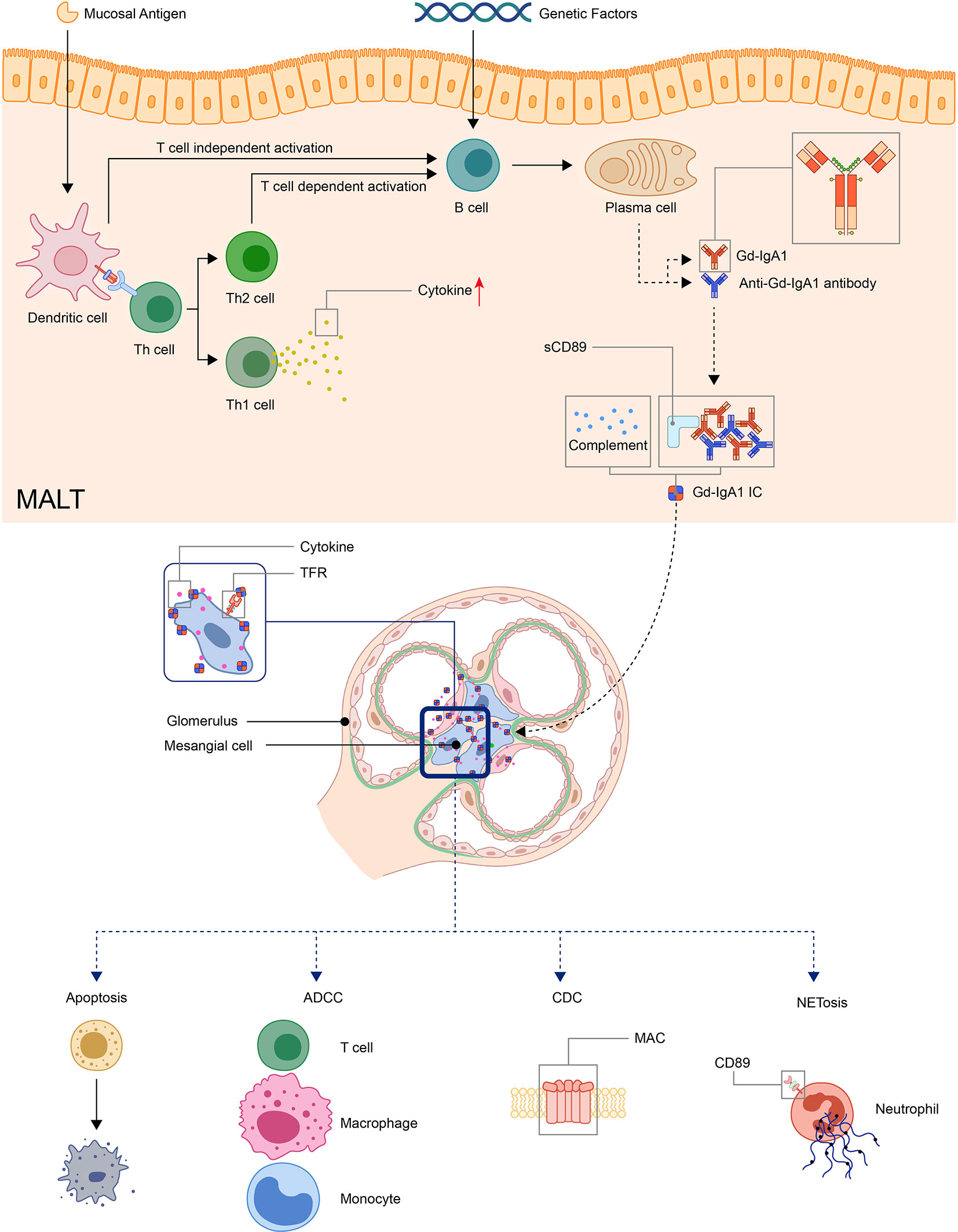
Hypothesized pathophysiological mechanism: exposure to allergen/antigen (e.g., infection, drugs) → stimulation of IgA production → deposition of IgA immune complexes in vascular walls (e.g., in the skin, GI tract, joints, kidneys) → activation of complement → vascular inflammation and damage
Clinical features
Key features
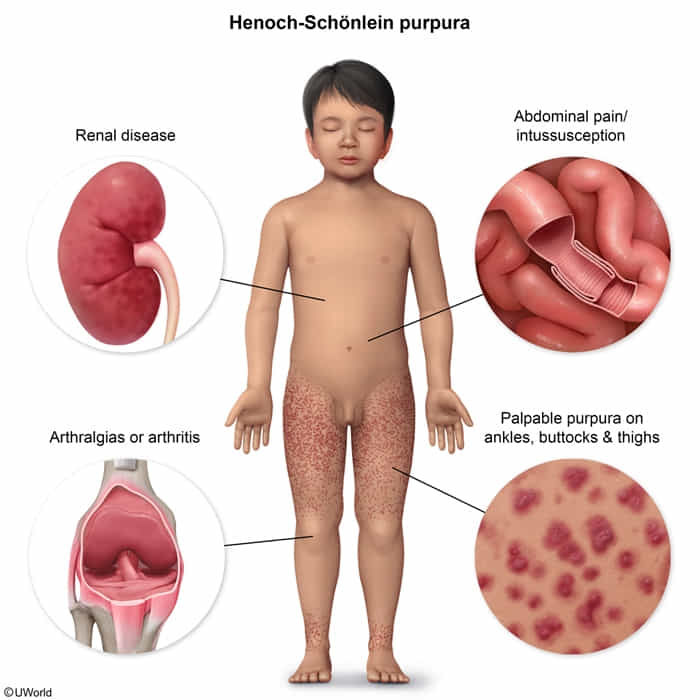
Triad of palpable purpura, arthralgias, and abdominal pain in children.
An upper respiratory tract infection often precedes symptom onset by 1–3 weeks.
Skin (∼ 100% of cases)
Symmetrically distributed erythematous papules or urticarial lesions that coalesce into palpable purpura
Bullae, pustules, and necrotic or hemorrhagic purpura (more common in adults)
Most commonly in the lower extremities, buttocks, and other areas of pressure or constraint (e.g., from clothing)
Joints (∼ 75% of cases)
Arthritis/arthralgia
Usually bilateral, self-limited, and nondestructive; children may present with a limp.
Most commonly in the ankles and knees
Gastrointestinal tract (∼ 60% of cases)
Colicky abdominal pain
Intussusception
Hematochezia or melena
Nausea and/or vomiting
Kidneys: IgA nephritis (20–50% of children; 50–80% of adults)