Two primary flexor tendons for each finger (index to small):
Flexor Digitorum Superficialis (FDS):
Inserts on the sides of the middle phalanx.
Action: Flexes the PIP joint.
To test: Hold other fingers in extension and ask pt to flex the finger being tested.
Flexor Digitorum Profundus (FDP):
Travels through the split in the FDS tendon (Camper’s chiasm).
Inserts on the base of the distal phalanx.
Action: Flexes the DIP joint.
To test: Stabilize the MCP and PIP joints and ask pt to flex the fingertip.
Avulsion of FDP tendon → Jersey finger.
Diseases
Mallet Finger (“Baseball Finger”)
Mechanism: Forced hyperflexion of an extended distal interphalangeal (DIP) joint.
Pathophysiology: Rupture or avulsion of the extensor tendon at its insertion on the distal phalanx.
Clinical Features: Pt cannot actively extend the DIP joint. The tip of the finger is flexed at rest.
Tx: Splinting the DIP joint in full extension for 6-8 weeks.
Boutonnière Deformity
Mechanism: Forced flexion of the proximal interphalangeal (PIP) joint, or a direct blow to the dorsum of the PIP.
Pathophysiology: Rupture of the central slip of the extensor tendon at the middle phalanx. Lateral bands slip volarly.
Clinical Features: Flexion of PIP joint and hyperextension of DIP joint.
Tx: Splinting the PIP joint in extension.
Swan Neck Deformity
Mechanism: Often associated with rheumatoid arthritis; can also be post-traumatic (volar plate injury).
Pathophysiology: Functional imbalance between extrinsic and intrinsic muscles leading to contracture.
Clinical Features: Hyperextension of PIP joint and flexion of DIP joint. (Opposite of Boutonnière).
Tx: Treat underlying cause (e.g., RA), physiotherapy, possible surgery.
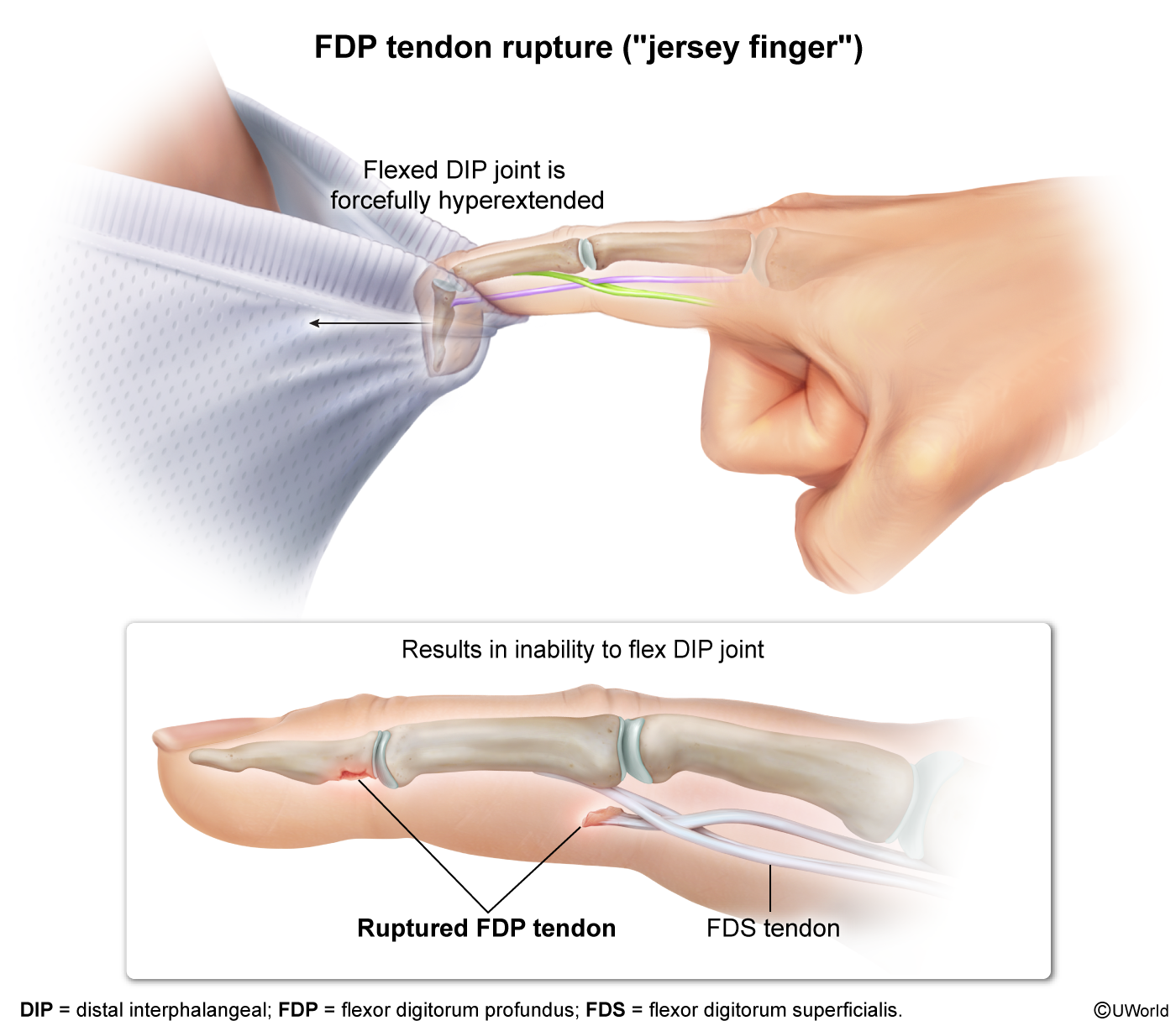
Jersey Finger
Mechanism: Forced hyperextension of a flexed DIP joint (e.g., grabbing an opponent’s jersey).
Pathophysiology: Avulsion/rupture of the flexor digitorum profundus (FDP) tendon from its insertion on the distal phalanx. Ring finger is most commonly affected.
Clinical Features: Pt cannot flex the DIP joint. When the pt makes a fist, the affected finger remains partially extended.
Tx: Requires surgical repair.
Gamekeeper’s Thumb (or Skier’s Thumb)
Mechanism: Forced abduction and hyperextension of the thumb (e.g., falling onto a ski pole).
Pathophysiology: Injury to the ulnar collateral ligament (UCL) of the thumb’s metacarpophalangeal (MCP) joint.
Clinical Features: Pain, swelling, and instability/laxity of the MCP joint with valgus stress. Weak pinch grasp.
Tx: Thumb spica splint/cast. Complete tears may require surgical repair.
Boxer’s Fracture
Mechanism: Direct impact with a clenched fist (e.g., punching a hard object).
Pathophysiology: Fracture of the neck of the 5th metacarpal.
Clinical Features: Pain, swelling over the ulnar side of the hand. Check for rotational deformity (finger “scissoring” when making a partial fist).
Tx: Ulnar gutter splint. Surgical pinning may be indicated for significant angulation.
Closed tendon injuries
Jersey finger
Affected tendon: flexor digitorum profundus (FDP); most commonly in the ring finger
Mechanism of injury
Sudden hyperextension of a flexed DIP joint (forced extension) → avulsion fracture and/or rupture of the FDP tendon at the insertion
Often seen when athletes grab an opponent’s jersey