Prevalence: most common type of acute compartment syndrome
Etiology
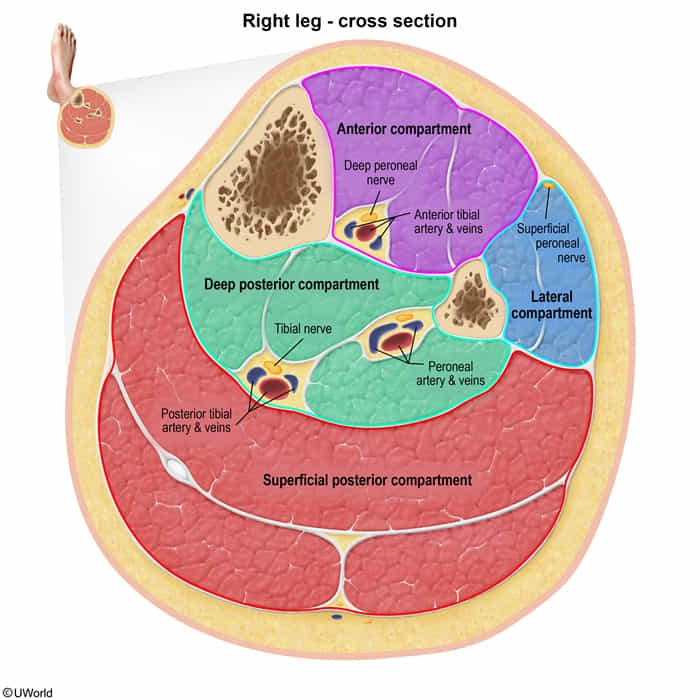
Usually due to trauma to the anterior compartment of the leg (e.g., tibial fracture)
Reperfusion: After vascular surgery or embolectomy (ischemia-reperfusion injury).
Clinical features
Early Sign: Pain out of proportion to injury (hallmark).
Key Exam Finding: Pain with passive stretch of the muscles in the affected compartment.
Late Signs (The 6 Ps): Paresthesia, Pallor, Poikilothermia, Paralysis, Pulselessness (Note: Pulses are often preserved until very late).
Palpable pulses are common. Compartment pressure occludes capillaries (microvasculature) first, causing muscle necrosis long before systolic arterial flow is blocked. Do not wait for pulselessness.c
Woody/Hard feeling: Tense, swollen compartment on palpation.