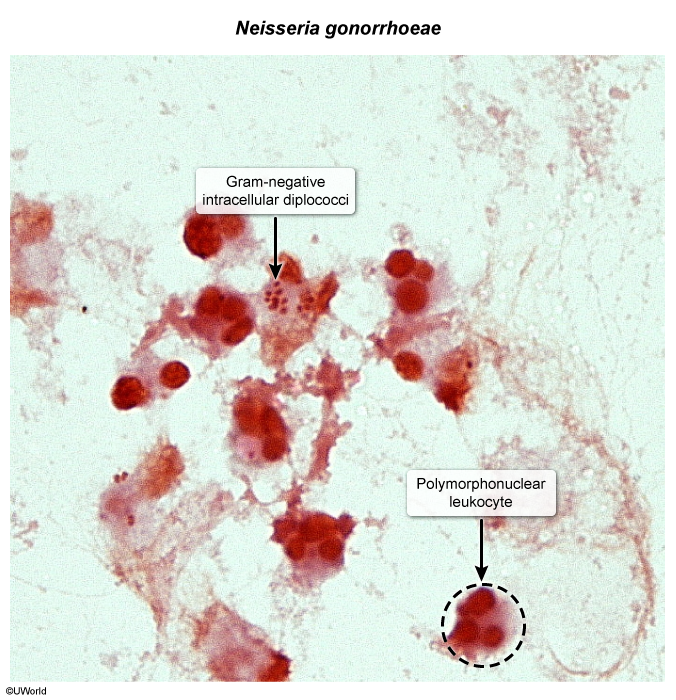
Gram stain: Gram-negative diplococci, often intracellular (within neutrophils).
Shape: Kidney-bean or coffee-bean shaped.
Metabolism: Aerobic.
Key enzyme: Oxidase-positive.
Culture: Grow on chocolate agar. For selective growth from non-sterile sites (e.g., genital), use Thayer-Martin agar (chocolate agar with Vancomycin, Polymyxin, and Nystatin - “VPN”).
Virulence Factor (shared): Pili for attachment, with high antigenic variation. tIgA protease cleaves secretory IgA.
Diagnosis: Lumbar puncture (LP) shows CSF with ↑ neutrophils, ↑ protein, ↓ glucose. Gram stain of CSF. Blood cultures.
Treatment: Ceftriaxone or Penicillin G.
Prophylaxis:
For close contacts: Rifampin, ciprofloxacin, or ceftriaxone. t
Goal of prophylaxis is to eradicate nasopharyngeal carriage of the bacteria to prevent it from invading the bloodstream or spreading to others.
Rifampin can penetrate extremely well into body fluids and tissues, specifically saliva, tears, and nasopharyngeal secretions. Hence its side effect: orange/red discoloration of body fluids
Vaccine: Conjugate vaccine against serotypes A, C, Y, W-135. Separate vaccine for serotype B.