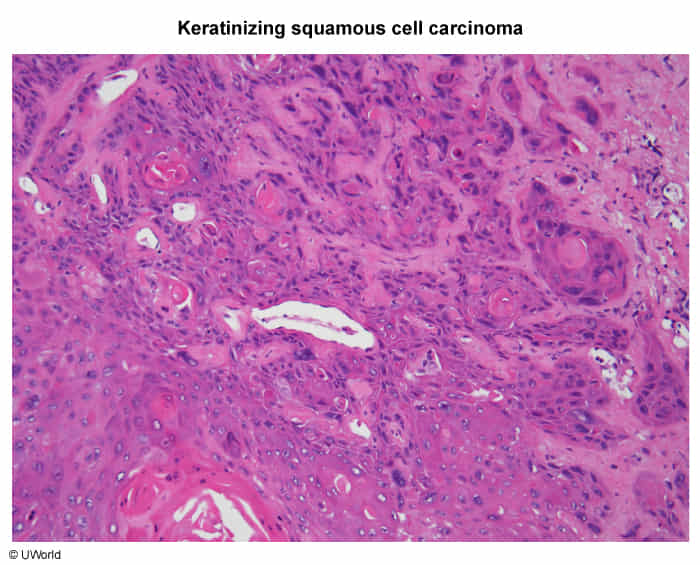
Definition: Malignant neoplasm of the oropharynx, which includes the tonsils, base of the tongue, soft palate, and pharyngeal walls. Over 90% are squamous cell carcinomas (SCC).
Two distinct etiologies:
HPV-Associated (70-80% of cases in North America/Europe): Primarily caused by HPV-16. The E6 oncoprotein inactivates p53, and the E7 oncoprotein inactivates Rb (retinoblastoma protein), leading to uncontrolled cell proliferation. Typically affects a younger demographic (4th-5th decade) and is associated with sexual behavior.
Non-HPV-Associated: Strongly linked to traditional risk factors like tobacco (smoking and smokeless) and alcohol use, especially in combination (synergistic effect). Tends to occur in an older population (6th-7th decade).
Field Cancerization: Widespread exposure of the upper aerodigestive tract to carcinogens (like tobacco) can lead to multiple independent primary tumors or a higher risk of recurrence.
Clinical Presentation
Often asymptomatic in early stages, leading to late diagnosis.
Most common presenting symptom: A persistent, painless neck mass (cervical lymphadenopathy), which is often cystic.
Referred otalgia (ear pain) via the glossopharyngeal nerve (CN IX).
Trismus (difficulty opening the mouth), muffled voice ("hot potato voice"), or dysarthria.
Unintentional weight loss.
Physical Exam: May reveal an ulcerative, indurated, or exophytic lesion, or a red/white patch (erythroplakia/leukoplakia) in the oropharynx.
Diagnosis
Initial Evaluation: Laryngoscopy and a thorough head and neck exam to visualize the primary tumor.
Gold Standard:Biopsy of the primary lesion for histopathologic confirmation.
HPV Testing: All newly diagnosed oropharyngeal SCCs should be tested for HPV, typically via p16 immunohistochemistry (IHC), which serves as a surrogate marker. This is crucial as HPV status is a major prognostic factor and determines the staging system used.
Staging:
CT with contrast of the neck and chest is the initial imaging modality to assess tumor extent and nodal/distant metastases.
PET/CT is superior for detecting regional and distant metastases.
Other Malignancies: Lymphoma (may present with nodal disease), metastatic disease from another primary site.
Management/Treatment
Treatment is complex and multidisciplinary, depending on the stage and HPV status.
Early-Stage (I-II): Single modality therapy, either surgery (e.g., transoral robotic surgery - TORS) or radiation therapy (RT).
Advanced-Stage (III-IV): Multimodality therapy is standard.
Primary Treatment: Concurrent chemoradiation (chemotherapy, often cisplatin-based, given with RT) is the most common approach.
Surgery may be used first, followed by adjuvant RT or chemoradiation, depending on risk factors.
Targeted Therapy/Immunotherapy: Agents like Cetuximab (EGFR inhibitor) or checkpoint inhibitors (e.g., Nivolumab) are options for recurrent or metastatic disease.
Key Associations/Complications
Prognosis: HPV-positive tumors have a significantly better prognosis and response to treatment compared to HPV-negative tumors. The 5-year survival is >80% for HPV-positive vs. <50% for HPV-negative cancers.
Complications of Treatment: Significant long-term morbidity from radiation includes xerostomia (dry mouth), mucositis, odynophagia (requiring feeding tube), and risk of osteoradionecrosis.
Second Primary Malignancy: Patients with HNSCC, especially those with tobacco/alcohol-related cancers, are at high risk for developing another primary tumor in the aerodigestive tract (e.g., lung, esophagus) due to field cancerization.