Reduced blood flow to the colon, leading to inflammation and injury. Most cases are due to non-occlusive ischemia (e.g., “low-flow” state like shock, heart failure, sepsis) rather than acute arterial occlusion.
Watershed areas are most vulnerable due to limited collateral blood supply.
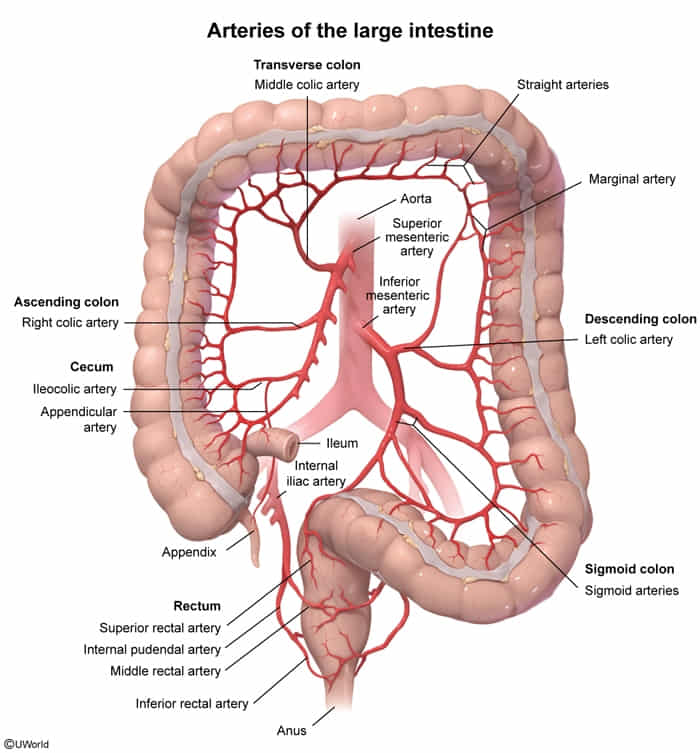
Splenic flexure (Griffith’s point): junction of SMA and IMA territories.
Rectosigmoid junction (Sudeck’s point): junction of IMA and iliac artery territories.
Risk factors: elderly age (>60), atherosclerosis, hypotension, heart failure, aortic surgery (esp. AAA repair with IMA ligation), vasculitis, hypercoagulable states.
Clinical Presentation
Classic triad: rapid onset of mild-to-moderate crampy abdominal pain (often left-sided), followed by hematochezia (bright red blood per rectum) or bloody diarrhea within 24 hours.
Nausea, vomiting, and diarrhea may also occur.
Peritoneal signs (rigidity, guarding) suggest transmural necrosis and perforation (a surgical emergency).
Diagnosis
CT scan with IV contrast is the best initial imaging test to rule out other causes of abdominal pain and support the diagnosis.
Severe findings: pneumatosis (gas in the bowel wall) or portal venous gas indicate infarction.
Colonoscopy is the gold standard for diagnosis, showing edematous, friable mucosa, petechial hemorrhages, and segmental erythema. It should be performed without aggressive insufflation to avoid perforation.
Labs are nonspecific but may show leukocytosis and elevated lactate in severe cases.
DDx (Differential Diagnosis)
Infectious colitis (e.g., C. difficile, E. coli O157:H7, Campylobacter): Differentiated by stool cultures and specific toxin assays. Often has more profuse watery diarrhea and fever.
Inflammatory Bowel Disease (IBD) (Ulcerative Colitis/Crohn’s): Onset is typically more gradual and chronic. Biopsy is key. UC pain is often LLQ, while Crohn’s is often RLQ.
Diverticulitis: Presents with LLQ pain and fever but usually without significant bleeding.
Acute mesenteric ischemia (AMI): Much more severe “pain out of proportion to exam,” often caused by an embolism to the SMA. Involves the small bowel. Requires angiography for diagnosis.
Management/Treatment
Most cases are transient and resolve with supportive care.
Bowel rest (NPO), IV fluids to restore perfusion, and correction of underlying causes.
Broad-spectrum antibiotics (e.g., piperacillin-tazobactam or a fluoroquinolone plus metronidazole) are given to prevent bacterial translocation and sepsis.
Surgical intervention (colectomy) is required for patients with signs of peritonitis, bowel gangrene, or perforation.
Key Associations/Complications
Complications: Gangrene, perforation, hemorrhage, and post-ischemic stricture formation.
Prognosis: Most patients recover fully with medical management. However, mortality is high if surgery is needed. Isolated right-sided colonic ischemia has a worse prognosis.
Chronic mesenteric ischemia
Pathophysiology
Atherosclerosis of Celiac, SMA, or IMA (usually requires ≥2 vessel occlusion).
“Intestinal Angina”: Blood flow insufficient for post-prandial metabolic demand.
Clinical Features
Postprandial pain: Dull epigastric pain ~30 min after eating.
Food fear (sitzophobia) & Weight loss.
Hx of CAD/PAD; abdominal bruit often present.
Diagnostics
CT Angiography (Preferred initial test).
Angiography (Gold standard).
Treatment
Revascularization: Stenting (endovascular) or Bypass (open).