Bile salts (aka bile acids, 50%): Most abundant solute. Amphipathic derivatives of cholesterol. Emulsify fats for digestion; absorb fat-soluble vitamins (A, D, E, K).
Crohn’s Disease / Terminal Ileum Resection: Disruption of enterohepatic circulation → ↓ bile salt reabsorption. t
Rapid weight loss: Mobilization of tissue cholesterol.
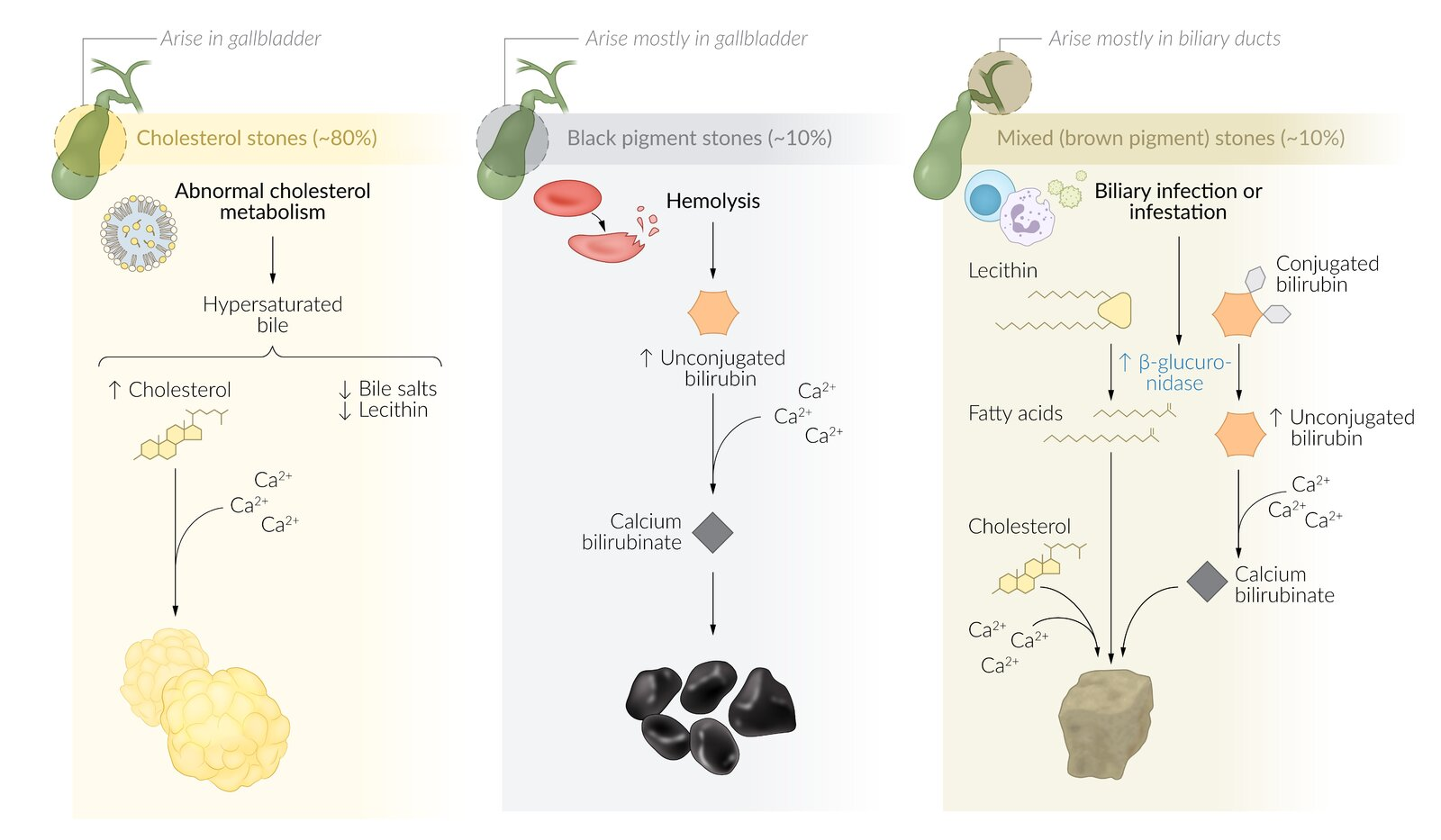
Black pigment stones
Associated with Chronic Hemolysis (e.g., Sickle Cell, Hereditary Spherocytosis) and Cirrhosis.
Mechanism: ↑ Unconjugated bilirubin load precipitates with calcium.
Typically Radio-opaque.
Mixed/brown pigment stones
Radiolucent
Risk factors: bacterial infections and parasites (e.g., Clonorchis sinensis, Opisthorchis species) in the biliary tract, sclerosing cholangitis
Pathophysiology: infection or infestation → release of β-glucuronidase (by injured hepatocytes and bacteria) → hydrolyzes conjugated bilirubin and lecithin in the bile → increased unconjugated bilirubin and fatty acids → precipitation of calcium carbonate, cholesterol, and calcium bilirubinate (dark color) in bile
Unconjugated bilirubin is lipid-soluble and insoluble in water. This insolubility allows it to precipitate with calcium ions, forming calcium bilirubinate. While conjugated bilirubin is water-soluble (bound to glucuronic acid) and remains dissolved in bile, preventing precipitation.
β-glucuronidase: a lysosomal enzyme that deconjugates direct bilirubin. Present in breast milk and can cause neonatal unconjugated hyperbilirubinemia. Also found in intestinal brush border cells, where it deconjugates direct bilirubin to release indirect bilirubin that is then reabsorbed and recycled. Bacterial β-glucuronidase in the biliary tract is implicated in the pathogenesis of brown pigment gallstones.
Pathophysiology
Clinical features
Diagnostics
Abdominal Ultrasound (US): Best initial and most accurate test for stones in the gallbladder.
Shows hyperechoic foci (stones) with a posterior acoustic shadow.
Labs: Typically normal in uncomplicated cholelithiasis. LFTs (ALP, GGT, bilirubin) will be elevated if a stone passes into the common bile duct (choledocholithiasis).
For suspected ductal stones (choledocholithiasis):
MRCP (Magnetic Resonance Cholangiopancreatography): Excellent non-invasive test to visualize the biliary and pancreatic ducts. Used to confirm suspected CBD stones before proceeding to an invasive procedure. Diagnostic only.
ERCP (Endoscopic Retrograde Cholangiopancreatography): Gold standard for both diagnosis and therapy of choledocholithiasis. Allows for sphincterotomy and stone extraction.
PTC (Percutaneous Transhepatic Cholangiography):Invasive imaging used when ERCP is unsuccessful or contraindicated. Can also be used for therapeutic biliary drainage.
HIDA Scan (cholescintigraphy): Primarily used to diagnose acute cholecystitis (not routine for cholelithiasis); shows non-visualization of the gallbladder.