Etiology
- Malignancy of primitive neural crest cells.
- Most common extracranial solid tumor of childhood. Median age at Dx is < 2 years.
- Arises from adrenal medulla (most common) or sympathetic ganglia.
- In adults, pheochromocytoma is the most common tumor of the adrenal medulla, while in children it is neuroblastoma.
- Associated with amplification of the N-myc oncogene (poor prognosis).
Pathophysiology
Clinical features
- Abdominal mass: Firm, irregular, and crosses the midline.
- Systemic Sx: Fever, weight loss, irritability.
- Metastatic signs:
- Periorbital ecchymoses (“raccoon eyes”) from orbital metastasis.
- Bone pain from bone marrow infiltration.
- Subcutaneous nodules (blueberry muffin baby).
- Paraneoplastic Syndromes:
- Opsoclonus-myoclonus syndrome (“dancing eyes, dancing feet”).
- Catecholamine secretion (less common than in pheochromocytoma): HTN, flushing, diarrhea.

Diagnostics
- Urine/Serum: ↑ homovanillic acid (HVA) and vanillylmandelic acid (VMA), which are breakdown products of catecholamines.
- Imaging (CT/MRI): Abdominal mass with calcifications and hemorrhage.
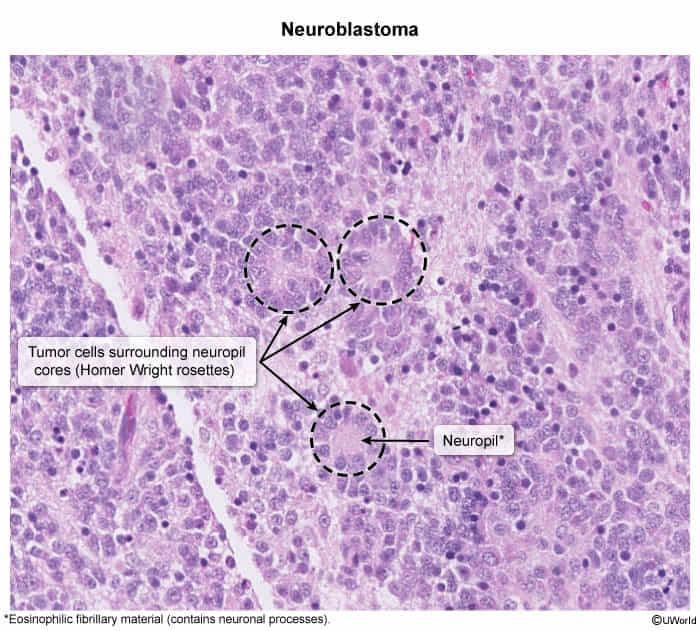
- Biopsy/Histology: Small, round blue cells forming Homer-Wright pseudorosettes.
- Bombesin and neuron-specific enolase (NSE) can be elevated tumor markers.
- MIBG scan (metaiodobenzylguanidine) is used to detect metastases.
Treatment