Epidemiology
Etiology
- Prolactin-secreting pituitary adenoma (prolactinomas)
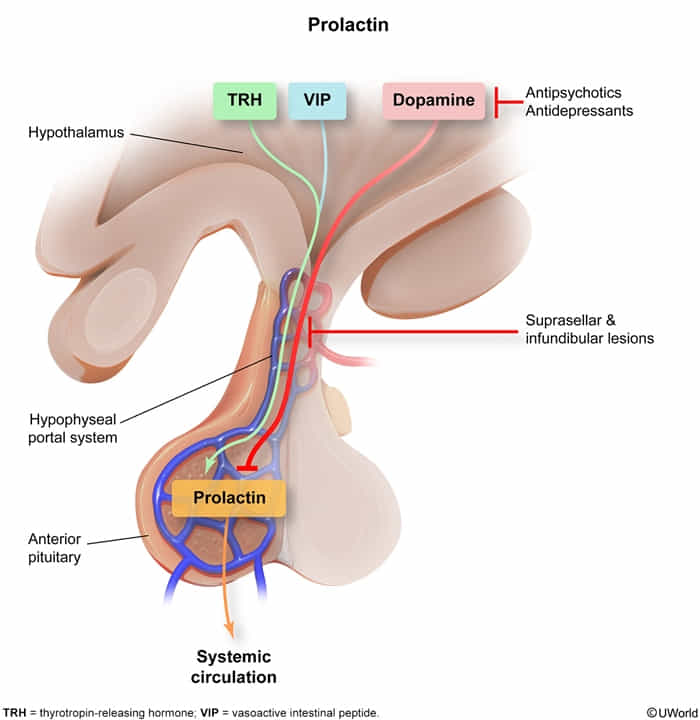
- Damage to the hypothalamus and/or infundibular stalk
- They compress the infundibular stalk and result in an interruption of the tonic inhibitory effect of hypothalamic dopamine on the secretion of prolactin
- They compress the infundibular stalk and result in an interruption of the tonic inhibitory effect of hypothalamic dopamine on the secretion of prolactin
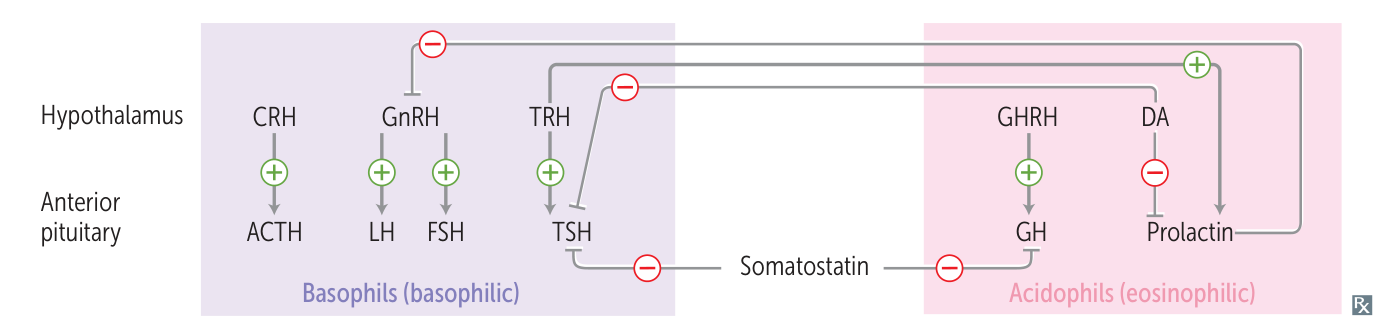
- Severe primary hypothyroidism: ↓ T3/T4 → ↑ TRH → ↑ prolactin t
- Drugs
- Dopamine antagonists:
- Antiemetics: metoclopramide, domperidone
- Antipsychotics (e.g., haloperidol, risperidone)
- Certain tricyclic antidepressants: e.g., clomipramine
- Dopamine antagonists:
- Physiological causes: stress, pregnancy, lactation, nipple stimulation, crying baby, sexual orgasm, sleep, exercise
Tip
The dopamine-prolactin pathway (tuberoinfundibular pathway) is unique among other pathways, as dopamine inhibits prolactin.
Pathophysiology
- ↑ Prolactin → galactorrhea
- ↑ Prolactin → suppression of GnRH → ↓ LH, ↓ FSH → ↓ estrogen, ↓ testosterone → hypogonadotropic hypogonadism
Clinical features
Male
- ↓ Testosterone
- Loss of libido, erectile dysfunction, infertility
- Gynecomastia
- Reduced facial and body hair
- Osteoporosis
Tip
Patients with hyperprolactinemia due to a pituitary adenoma may also present with bitemporal hemianopsia and headache.
Female
- Premenopausal women: oligomenorrhea/amenorrhea, infertility, galactorrhea, hot flashes, decreased bone density
- Postmenopausal women: mass-effect symptoms (headache, visual field defects)
Diagnostics
Treatment
- Ergot dopamine agonists (treatment of choice): bromocriptine, cabergoline
- Non-ergot dopamine agonists (Ropinirole, Pramipexole, Apomorphine, Rotigotine) are not used here