- Patho/Etiology
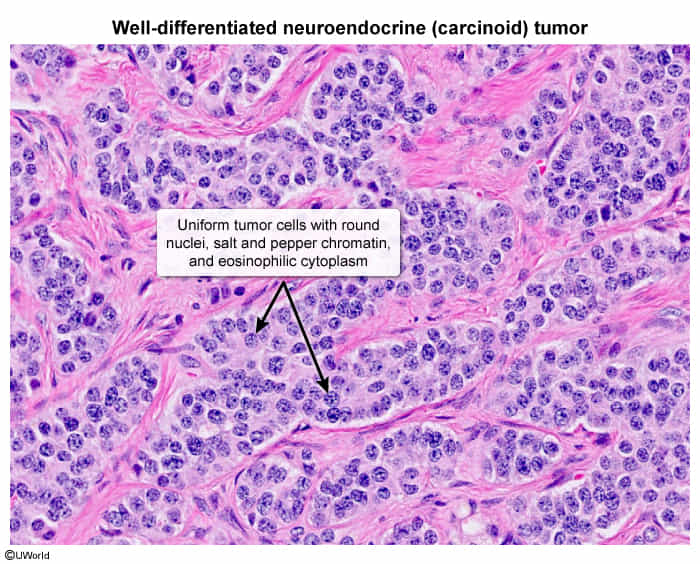
- Well-differentiated neuroendocrine tumors derived from enterochromaffin cells.
- Slow-growing but have malignant potential.
- Most common sites: Gastrointestinal tract (especially ileum and appendix) and lungs (bronchial carcinoids).
- Gross appearance is typically yellow or tan.
- Clinical Presentation
- Many are asymptomatic and found incidentally.
- Symptoms can arise from mass effect (e.g., bowel obstruction, appendicitis) or hormone secretion.
- Carcinoid Syndrome: Occurs when vasoactive substances (primarily serotonin) secreted by the tumor enter systemic circulation, bypassing hepatic first-pass metabolism. This typically implies metastasis to the liver.
- Classic Triad of Carcinoid Syndrome:
- Flushing: Episodic, cutaneous flushing of the face and neck, often triggered by alcohol, stress, or certain foods.
- Diarrhea: Secretory, watery diarrhea.
- Wheezing: Bronchospasm.
- Carcinoid Heart Disease: Fibrotic plaques develop on the endocardium, predominantly affecting right-sided heart valves (tricuspid regurgitation, pulmonic stenosis). The left side is spared because the lungs metabolize serotonin (via monoamine oxidase). t
- Pellagra: Can occur due to diversion of dietary tryptophan to synthesize serotonin, leading to niacin (B3) deficiency (dementia, dermatitis, diarrhea).
- Diagnosis
- Labs: Best initial test is a 24-hour urine for 5-hydroxyindoleacetic acid (5-HIAA), a serotonin metabolite. Serum chromogranin A is a sensitive tumor marker.
- Imaging: CT or MRI to localize the tumor and assess for metastases. OctreoScan (somatostatin receptor scintigraphy) is highly specific for localizing tumors because carcinoid cells express somatostatin receptors.
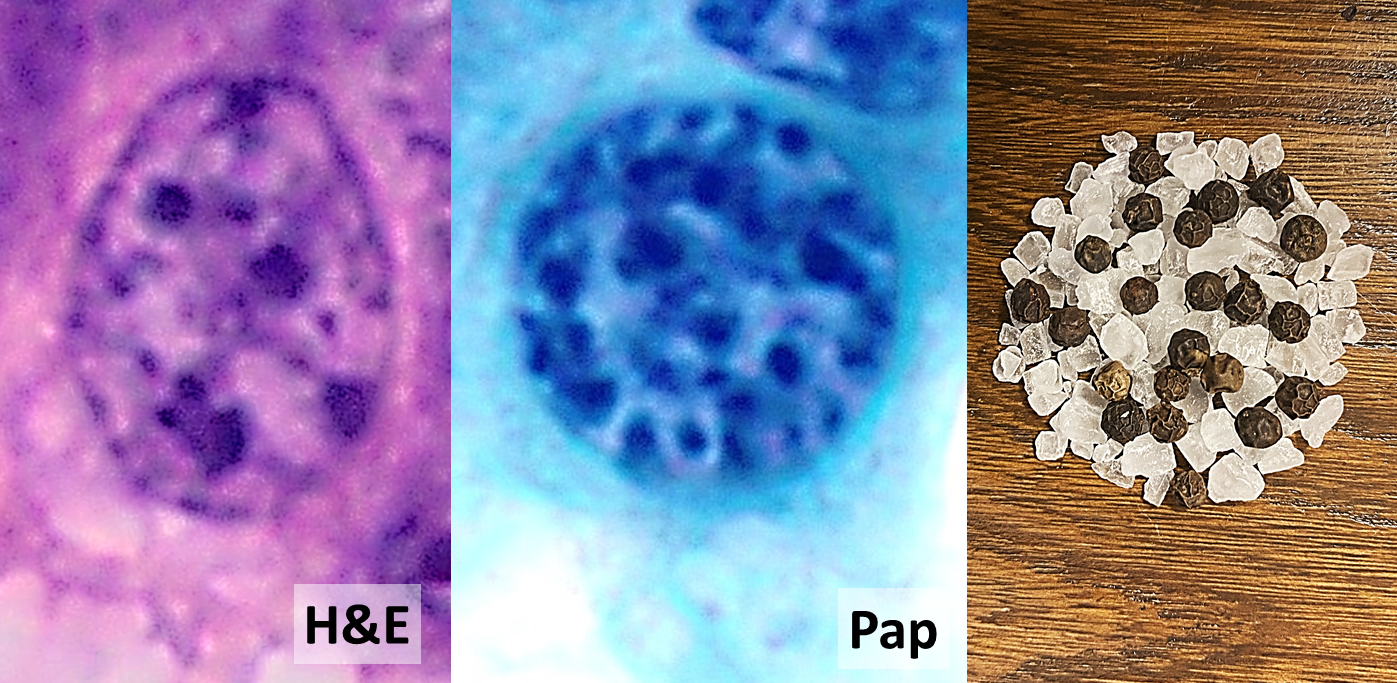
- Histology: Monotonous, round cells with “salt-and-pepper” chromatin, often arranged in nests or rosettes. Tumors stain positive for chromogranin A and synaptophysin.
- Differential diagnostics
- Irritable Bowel Syndrome (IBS): Can present with abdominal pain and diarrhea, but lacks flushing, wheezing, and the specific biochemical markers.
- Asthma: Presents with wheezing but not typically associated with flushing or diarrhea.
- Menopause: Causes flushing but is not associated with the other systemic symptoms of carcinoid syndrome.
- Pellagra (Niacin Deficiency): Presents with dermatitis, diarrhea, and dementia, but lacks flushing and wheezing.
- Other Neuroendocrine Tumors (NETs): Such as Zollinger-Ellison syndrome or VIPoma, which have specific hormone profiles and presentations (e.g., severe peptic ulcers, watery diarrhea without flushing).
- Management
- Surgery: Resection is the only curative treatment for localized tumors.
- Symptom control (Carcinoid Syndrome):
- Octreotide (a somatostatin analog) is the mainstay of therapy. It inhibits the secretion of hormones from the tumor, controlling flushing and diarrhea.
- Advanced/Metastatic Disease:
- May involve chemotherapy, though its effectiveness can be limited.
- Peptide Receptor Radionuclide Therapy (PRRT): A targeted radiation therapy for tumors that express somatostatin receptors.
- Key Associations/Complications
- Carcinoid Crisis: A life-threatening event with profound flushing, hypotension, and bronchoconstriction, often precipitated by surgery, anesthesia, or stress.
- Right-sided cardiac valvular disease is a major cause of morbidity and mortality.
- Most common tumor of the appendix.