Emotional/physical stress → activation of the sympathetic nervous system → massive catecholamine discharge → cardiotoxicity, multivessel spasms, and dysfunction → myocardial stunning
A state of abnormal regional LV wall motion that persists for hours to weeks following transient ischemia
Clinical features
Patients typically have chest pain that can mimic a myocardial infarction and may also have symptoms of heart failure (eg, dyspnea, lower extremity swelling).
ECG often shows evidence of ischemia (eg, ST elevation, T-wave inversion) in the anterior precordial leads; however, coronary angiography typically reveals an absence of obstructive coronary artery disease. c
The condition usually resolves within several weeks with supportive treatment only.
Diagnostics
Initial: ECG (ST-segment elevation, often anterior leads; deep T-wave inversions). Indistinguishable from STEMI.
Key Labs: (+) Troponins (usually mild/moderate elevation, disproportionately low vs. extent of wall motion abnormality), ↑ BNP.
Mechanism: Differential β-Adrenergic Receptor Density
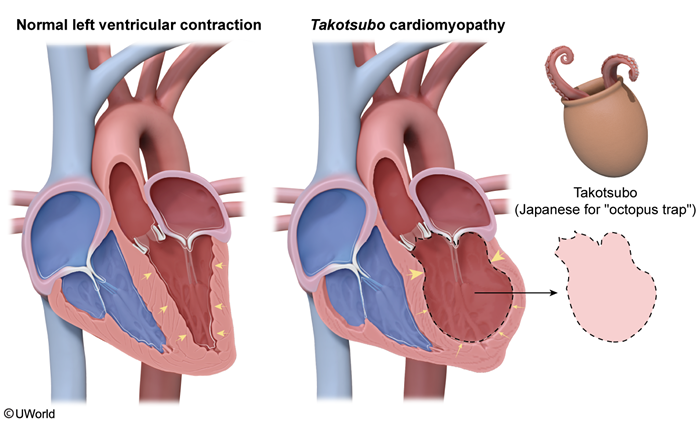
Anatomic Gradient: The cardiac apex has the highest density of β-adrenergic receptors; the base has the lowest.
Catecholamine Toxicity: Massive sympathetic surge triggers a protective molecular switch (Gs→Gi pathway) in the receptor-dense apex, causing acute negative inotropy (stunning).
Basal Sparing: The base has fewer receptors, escapes toxicity, and hypercontracts to compensate for the failed apex.
Confirmatory/Gold Standard: Coronary Angiography. Mustshow patent coronary arteries (no obstructive CAD) to rule out ACS. Ventriculography confirms shape. c
Mayo Clinic Criteria: 1) Transient LV dysfunction (apical ballooning), 2) Absence of obstructive CAD, 3) New ECG changes/Trop leak, 4) No pheochromocytoma/myocarditis.
Treatment
Acute Stabilization: Treat as ACS (ASA, heparin, nitrates) until obstructive CAD ruled out via cath.
Supportive Care (Mainstay):
HF Mgmt: Diuretics (furosemide) for volume overload.
GDMT: Beta-blockers (blunt catecholamines), ACEi/ARBs (prevent remodeling) until LVEF recovers.
Thromboembolism Prophylaxis: Anticoagulation if LV thrombus identified on echo (high risk due to stasis in apex).
Avoid: Inotropes if LVOT obstruction present (worsens gradient).