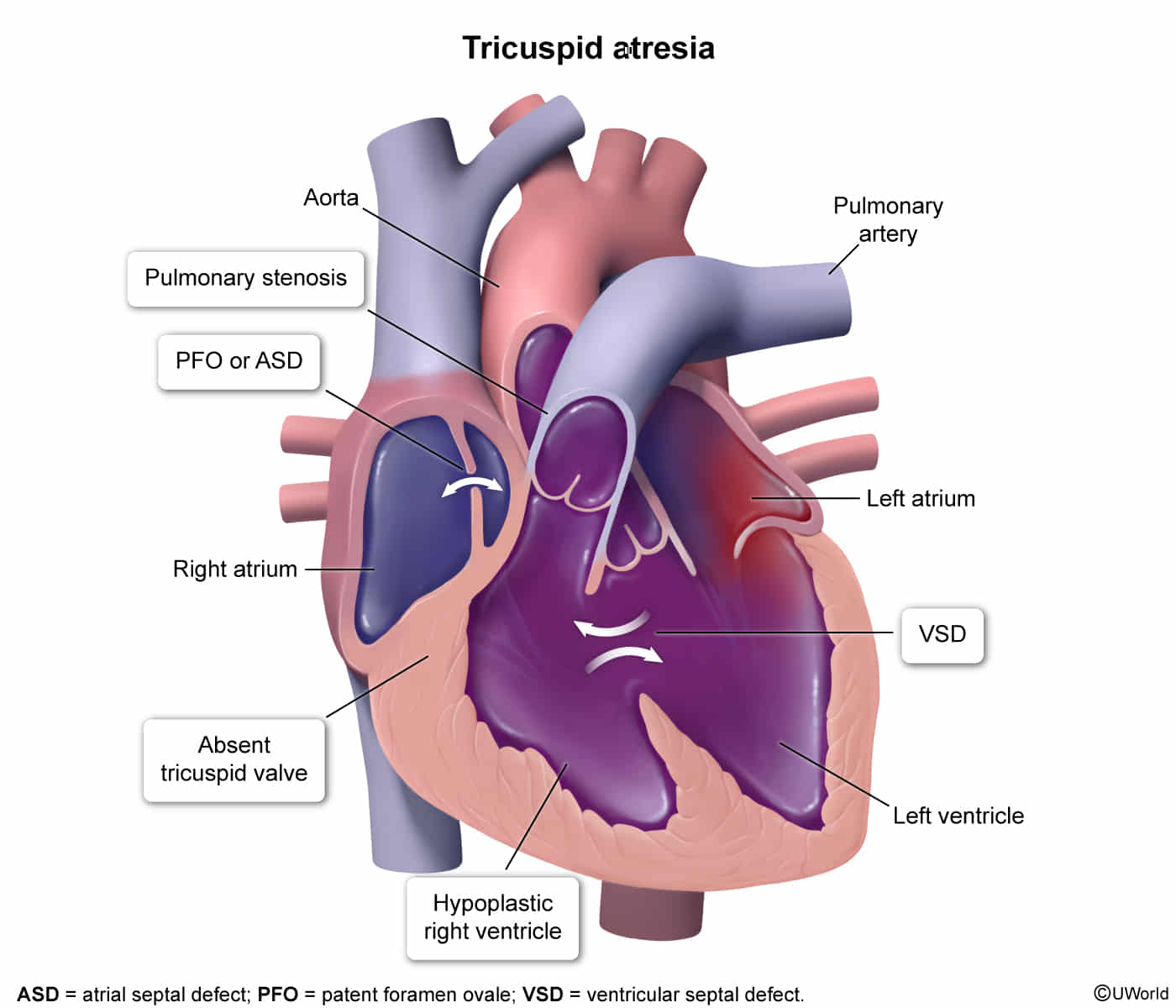
Tricuspid Valve Atresia (TVA)
- Epidemiology & Pathophysiology
- Congenital agenesis of the tricuspid valve No communication between RA and RV.
- Hypoplastic RV (underdeveloped).
- Survival depends on obligatory R L shunt (ASD/PFO) for mixing and VSD or PDA for pulmonary blood flow.
- 3rd most common form of cyanotic CHD.
- Clinical Features
- Cyanosis: Present at birth or shortly after (severity depends on magnitude of pulmonary blood flow).
- Heart Sounds:
- Single S2 (pulmonary valve usually involved/hypoplastic).
- Holosystolic murmur at LLSB (due to VSD) is common.
- Symptoms: Tachypnea, poor feeding, hypoxic spells (if pulmonary flow is restricted).
- Diagnosis
- ECG (High-Yield):
- Left Axis Deviation (LAD).
- Left Ventricular Hypertrophy (LVH) (Since RV is hypoplastic, LV does all the pumping).
- Note: Most other cyanotic CHDs (e.g., TOF) show RAD and RVH.
- Tall, peaked P waves (RA enlargement). c
- CXR:
- Decreased pulmonary vascular markings (oligemia). c
- Heart size normal or slightly enlarged; R heart border rounding (RAE).
- Echocardiogram (Confirmatory/Gold Standard):
- Demonstrates absence of tricuspid valve.
- Hypoplastic RV.
- Presence of ASD/VSD/PDA.
- ECG (High-Yield):
- Differential Diagnostics
- Tetralogy of Fallot (TOF): Diff by ECG (RAD, RVH) and CXR (“Boot-shaped heart”).
- Ebstein Anomaly: Displacement of TV leaflets (not atresia). Diff by CXR (“Wall-to-wall” heart/Box-shaped), ECG (WPW association, RBBB).
- Transposition of Great Arteries (TGA): Diff by “Egg-on-string” CXR, severe cyanosis within hours, ECG (RAD).
- Total Anomalous Pulmonary Venous Return (TAPVR): Diff by “Snowman” sign on CXR, ECG (RAD).
- Pulmonary Atresia with Intact Ventricular Septum: Clinical picture very similar to TVA (hypoplastic RV + LAD on ECG); distinguished by Echo.
- Management
- Immediate Stabilization:
- IV Prostaglandin E1 (PGE1): Critical first step to maintain PDA and ensuring pulmonary blood flow.
- Surgical Repair (Staged Palliative Pathway):
- Neonatal: Systemic-to-pulmonary shunt (e.g., Blalock-Taussig shunt) or PA banding (if excessive flow).
- 4-6 Months: Bidirectional Glenn procedure (SVC connected to Pulmonary Artery).
- 2-4 Years: Fontan procedure (IVC connected to Pulmonary Artery).
- End Goal: Passive venous return to lungs; Single ventricle (LV) pumps oxygenated blood to body.
- Immediate Stabilization:
- Complications
- Paradoxical Emboli (Stroke risk due to R L shunting).
- Arrhythmias (Atrial flutter/fib due to RA dilation/scarring).
- Post-Fontan:
- Protein-Losing Enteropathy (PLE).
- Plastic Bronchitis.
- Thrombosis.
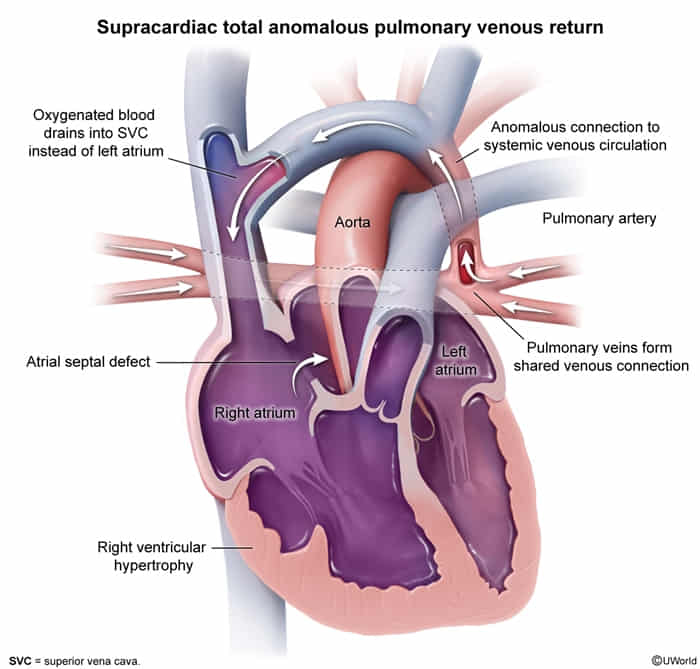
Total Anomalous Pulmonary Venous Return (TAPVR)
-
Epidemiology & Pathophysiology
- Mech: All 4 pulm veins drain into systemic venous circ (SVC, RA, Coronary Sinus) instead of LA.
- Requirement: Must have ASD or PFO for R→L shunt to sustain life (mixed blood → systemic).
- Class: Cyanotic Congenital Heart Disease (R→L shunt physiology).
-
Clinical Features
- Presentation varies by obstruction
- Obstructed (Infrastructure usually): Severe cyanosis/respiratory distress at birth (Pulm Edema). Sick neonate.
- Non-obstructed: Mild cyanosis, HF sxs (tachypnea, poor feeding) in infancy (weeks-months).
- Physical Exam:
- Heart Sounds: Fixed split S2 (due to RV volume overload/ASD).
- Murmur: Systolic ejection murmur at LUSB (increased flow across pulm valve). Diastolic rumble(increased flow across tricuspid).
- Signs of HF: Hepatomegaly, RV heave.
-
Diagnosis
- Initial/Screening:
- CXR:
- “Snowman” sign (or Figure-of-8): Dilated SVC + Vertical Vein + Cardiac shadow. Note: Often not seen in neonates due to thymus.
- Increased pulm vascular markings (pulm congestion).
- ECG: RAD, RVH (RV volume overload).
- CXR:
- Confirmatory/Gold Standard:
- Echocardiogram: Visualizes confluent vein behind LA; veins not entering LA. Dilated RA/RV.
- Other:
- Cardiac Cath: Only if Echo inconclusive (rarely needed). Shows O2 sat step-up in RA/SVC.
- Initial/Screening:
-
Differential Diagnostics
- RDS (Respiratory Distress Syndrome): Preterm, ground-glass on CXR. No fixed split S2.
- Transposition of Great Arteries (TGA): “Egg on a string” CXR. Cyanosis immediate.Single S2.
- Tetralogy of Fallot: “Boot-shaped heart”. VSD murmur. Cyanosis depends on RVOT obstruction degree (“Tet spells”).
- Persistent Pulm HTN of Newborn (PPHN): Structurally normal heart, severe hypoxemia.
-
Management
- Stabilization (ABC):
- O2, intubation if resp failure.
- Inotropes for HF.
- PGE1 (Prostaglandin): Usually not helpful (unlike ductal-dependent lesions like Coarctation or TGA) unless obstruction is severe and systemic flow is compromised, but rarely main mgmt.
- ECMO: If severe hypoxia/instability pre-op.
- Surgical Repair (Definitive):
- Obstructed: Emergent surgery.
- Non-obstructed: Elective but prompt repair (prevent pulm HTN).
- Procedure: Anastomosis of common pulm vein to LA; closure of ASD.
- Stabilization (ABC):
-
Complications
- Pulmonary Vein Stenosis (post-op).
- Arrhythmias (atrial).
- Pulmonary HTN (if repair delayed).