Pathophysiology & Classification
Central Cyanosis : ↓ Arterial O2 saturation (SaO2) or abnormal Hb. Deoxygenated Hb > 5 g/dL. Manifests in lips, tongue, mucous membranes.Peripheral Cyanosis : Normal SaO2, but ↑ tissue O2 extraction due to sluggish capillary flow. Manifests in distal extremities (fingers, toes), nose, earlobes.
Epidemiology & Risk Factors
Central : Cardiopulmonary dz (COPD, ILD, congenital heart dz), altitude, toxins (dapsone, local anesthetics, nitrates).Peripheral : Cold exposure, low cardiac output states (HF, shock), vasospasm (Raynaud’s), vascular occlusion.
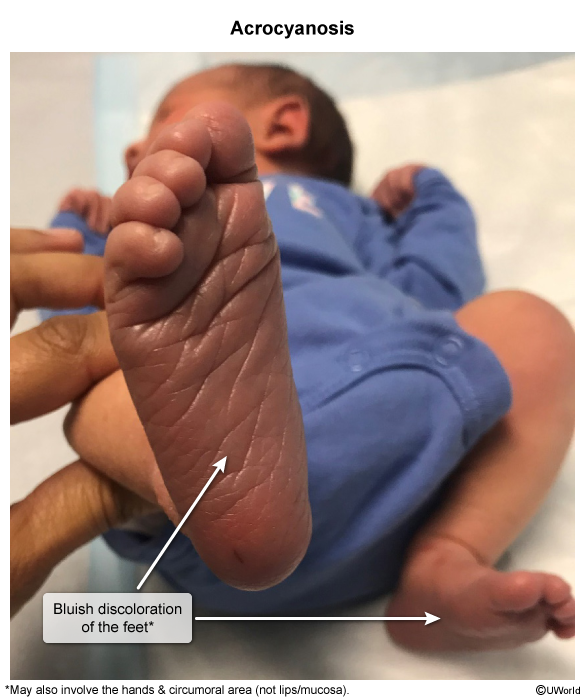
Acrocyanosis
Epidemiology & Risk Factors
Physiologic: Healthy newborns (resolves in days). c
Exaggerated autonomic/sympathetic response to the sudden drop in ambient temperature (womb vs. room air) causes reflex peripheral vasoconstriction.
Primary: Young women, low BMI. Triggered by cold/stress.
Secondary: Anorexia, POTS, CTDs, sympathomimetics.
Clinical Features
Persistent, symmetric blue/purple hands & feet.
Painless (key identifier).Cool, clammy extremities w/ normal pulses .
Diagnosis
Initial : Clinical H&P.Key Labs : Pulse ox normal (rules out central cyanosis).Confirmatory : None. Workup (ANA, CBC) only if atypical/secondary suspected.
Differential Diagnostics
Raynaud Phenomenon : Painful , episodic, triphasic color change (white → → Central Cyanosis : Involves mucosa (lips/tongue), ↓ SpO2.Acute Limb Ischemia : Painful, pulseless, pale (6 Ps).
Management
First-line : Reassurance.Conservative : Avoid cold, wear warm clothing.Refractory : CCBs (rarely needed).
Complications
Benign. No tissue necrosis or ulcers. Primarily cosmetic.