- Epidemiology & Risk Factors
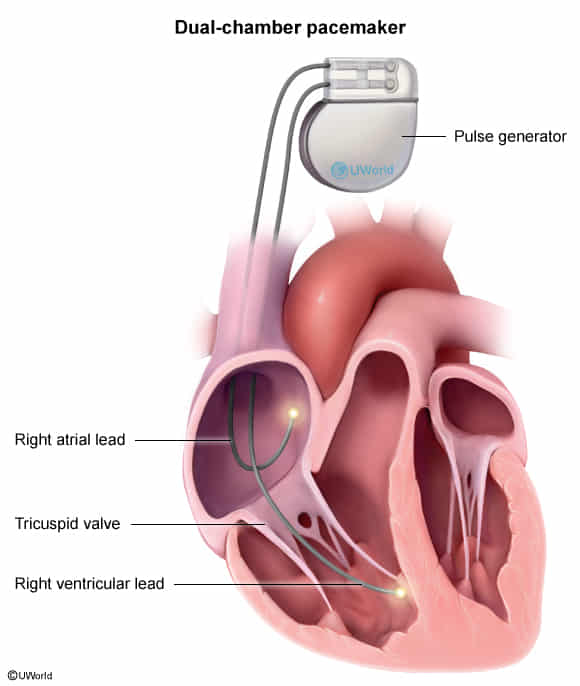
- Categories: Includes Permanent Pacemakers (PPM), Implantable Cardioverter-Defibrillators (ICD), and Cardiac Resynchronization Therapy (CRT / Biventricular pacemakers).
- Population: Primarily older adults w/ advanced structural heart disease, conduction abnormalities, or inherited channelopathies (e.g., Long QT, Brugada).
- Risk Factors for CIED Complications:
- Infections: DM, ESRD, corticosteroid use, early pocket re-exploration, pocket hematoma.
- Lead dislodgement: Advanced age, cognitive impairment (Twiddler’s syndrome).
- Clinical Features
- Presentations Requiring CIEDs: Syncope (due to AV block/VT/VF), symptomatic bradycardia, chronotropic incompetence, severe HF symptoms (NYHA II-IV) despite guideline-directed medical therapy (GDMT).
- Symptoms of Device Malfunction/Complication:
- Inappropriate shocks: Sudden, painful jolt in the chest without preceding lightheadedness (often due to AFib w/ RVR).
- Pocket infection: Localized erythema, swelling, tenderness, purulent drainage.
- CIED Endocarditis: Fever, chills, systemic toxicity, new tricuspid murmur.
- Pacemaker Syndrome: Fatigue, dizziness, palpitations, and visible neck vein pulsations (cannon A waves) due to AV dyssynchrony.
- Diagnosis
- Initial/Screening:
- EKG: Assesses pacing spikes (atrial vs. ventricular), underlying rhythm, capture failure, or oversensing.
- CXR: Evaluates lead position, lead fracture, or post-op complications (pneumothorax).
- Confirmatory/Gold Standard: Device Interrogation (identifies battery life, lead impedance, sensing thresholds, and logs of arrhythmias/shocks).
- Key Labs/Imaging (Infection Suspicion): Blood cultures (always draw before Abx), TEE (superior to TTE for evaluating lead vegetations/tricuspid valve).
- Differential Diagnostics (Differentiating Device Indications)
- PPM vs. ICD vs. CRT:
- PPM: Treats bradyarrhythmias (e.g., symptomatic sinus node dysfunction, Mobitz II 2nd-degree AV block, 3rd-degree AV block). Does not shock.
- ICD: Prevents sudden cardiac death (SCD) from tachyarrhythmias (VT/VF). Incorporates pacing functions.
- CRT: Treats HF by resynchronizing LV/RV contraction (biventricular pacing). Usually combined with an ICD (CRT-D).
- Appropriate vs. Inappropriate Shock:
- Appropriate: Device triggered by life-threatening VT/VF.
- Inappropriate: Device triggered by T-wave oversensing, SVT, or AFib w/ RVR. Diff by interrogation.
- Management
- Primary Prevention ICD Criteria:
- LVEF ≤ 35% + NYHA II-III HF symptoms + expected survival > 1 yr.
- LVEF ≤ 30% + post-MI (> 40 days) + NYHA I.
- Secondary Prevention ICD Criteria: Prior hemodynamically unstable VT or VF arrest.
- CRT Criteria: LVEF ≤ 35% + NYHA II-IV HF symptoms + LBBB with QRS ≥ 150 ms.
- Infection Management:
- Pocket infection or Endocarditis: Complete system extraction (leads + generator) + prolonged IV Abx (often covering S. aureus and S. epidermidis). Do not salvage the device.
- Perioperative/Procedural Management:
- Electrocautery can cause electromagnetic interference (EMI), leading to inappropriate shocks.
- Place a clinical magnet over the ICD during surgery above the umbilicus: temporarily suspends tachy-therapies (shocks) but leaves pacing intact (reverts to asynchronous pacing mode).
- Complications
- Acute (Peri-procedural): Pneumothorax, hemothorax, myocardial perforation (causing pericardial effusion/tamponade), pocket hematoma.
- Mechanical: Lead dislodgement, lead fracture, Twiddler’s syndrome (patient subconsciously rotates the generator in the pocket, wrapping/dislodging the leads).
- Infectious: CIED endocarditis (predominantly right-sided/tricuspid valve), pocket infection.
- Vascular: Subclavian vein thrombosis (presents w/ ipsilateral upper extremity swelling), tricuspid regurgitation c