-
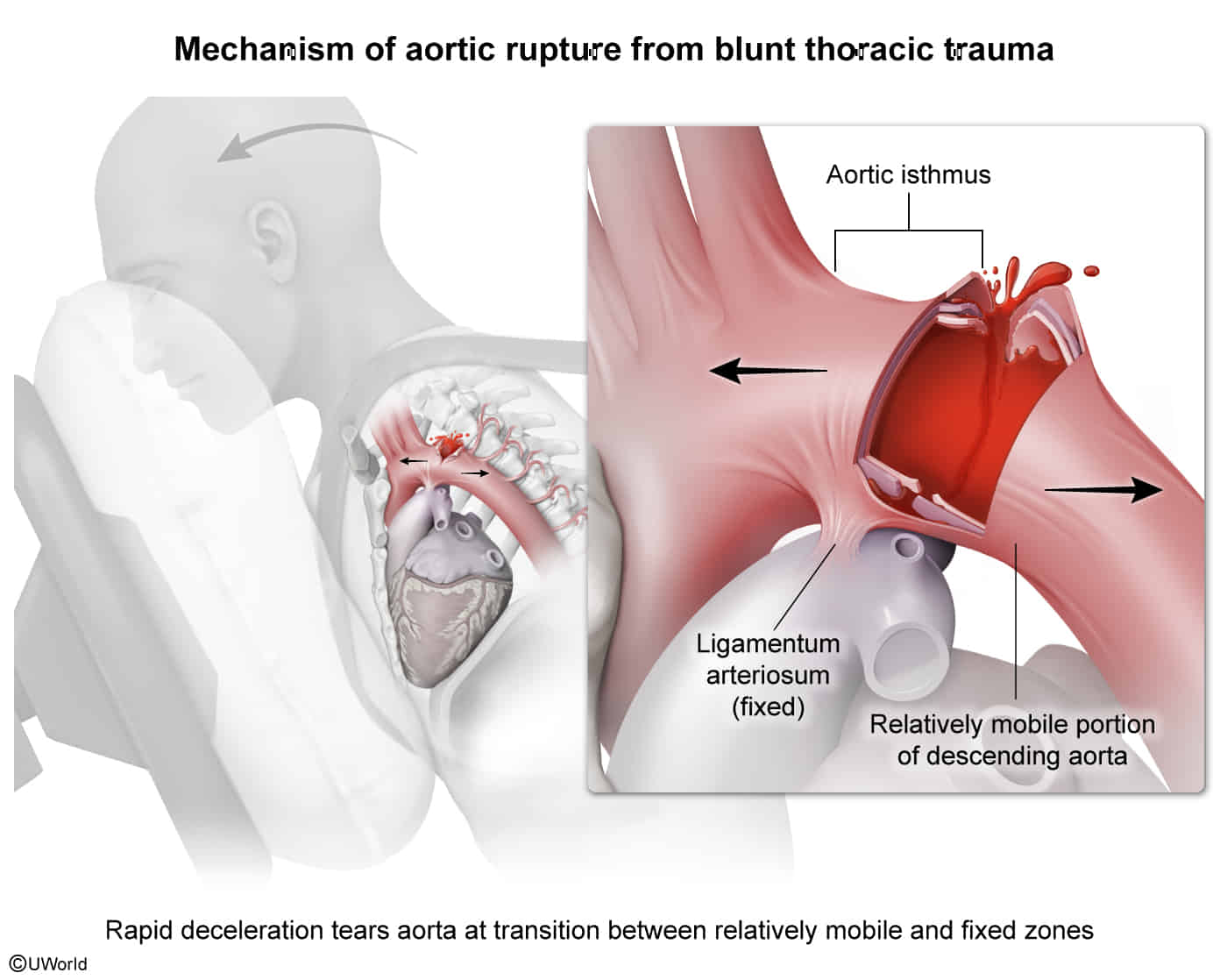
Definition: an injury of the thoracic aorta resulting from blunt trauma; most commonly occurs distal to the left subclavian artery in the aortic isthmus (between Aortic arch and descending aorta)
-
Etiology
- High-energy, rapid deceleration trauma (e.g., severe MVC, falls > 10 ft, pedestrian vs. auto).
- Typically involves the aortic isthmus (most common site) due to tethering by the ligamentum arteriosum.
- Most cases result in pre-hospital death (complete rupture); those surviving to the ED usually have a contained incomplete tear (adventitia intact).
-
Clinical features: Severity ranges from intimal lesions (e.g., aortic pseudocoarctation) to thoracic aortic rupture.
- May be asymptomatic or masked by distracting injuries.
- Tearing chest or back pain.
- Pseudocoarctation syndrome: Upper extremity hypertension with diminished/absent lower extremity pulses. c
- Discrepancy in BP between arms.
- Hoarseness (stretching/compression of the left recurrent laryngeal nerve). c
- Dysphagia or stridor (esophageal/tracheal compression by expanding hematoma).
-
Imaging
- Initial/Screening: Chest X-Ray (CXR) (AP view often done in trauma bay).
- Findings: Widened mediastinum (most sensitive), obscured aortic knob, left apical cap (blood over apex), rightward tracheal deviation, depression of left mainstem bronchus.
- Confirmatory/Gold Standard (Stable Pt): CT Angiography (CTA) of the chest. Highly sensitive and specific.
- Confirmatory (Unstable Pt/In OR): Transesophageal Echocardiography (TEE). Used when pt cannot be transported to CT scanner.
- Initial/Screening: Chest X-Ray (CXR) (AP view often done in trauma bay).
-
Management
- Initial Stabilization (ABCs): Assess for concurrent life-threatening hemorrhage.
- Anti-impulse Therapy (Medical Management): If pt is stable and NOT bleeding elsewhere, initiate strict HR and BP control to prevent extension/rupture of the tear.
- First-line: IV Beta-blockers (e.g., Esmolol). Target HR < 100 bpm and SBP < 100 mmHg.
- Add vasodilators (e.g., Nitroprusside) ONLY after HR is controlled (to prevent reflex tachycardia).
- Definitive Repair:
- Thoracic Endovascular Aortic Repair (TEVAR): Procedure of choice for Grade II-IV injuries. Associated with lower mortality and paraplegia rates compared to open repair.
- Open Surgical Repair: Reserved for cases where TEVAR is anatomically contraindicated.
- Note: Grade I injuries (small intimal tears) are often managed medically with serial CTA.