- Types & Anatomy
- Lateral Sprains (~85%):
- Mechanism: Inversion + Plantarflexion.
- Ligaments involved (in order of injury):
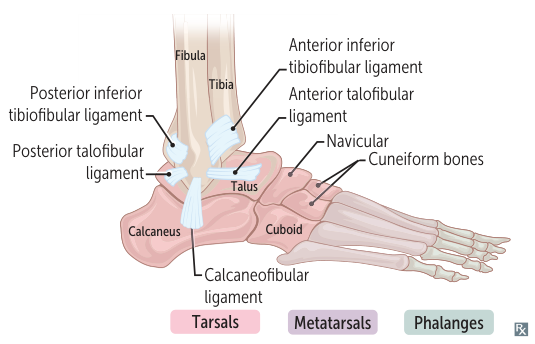
- Anterior Talofibular Ligament (ATFL): Most common; weakest.
- Calcaneofibular Ligament (CFL): Involved in more severe injuries. t
- Posterior Talofibular Ligament (PTFL): Rarely injured; only in severe dislocation.
- Medial Sprains:
- Mechanism: Eversion (forced external rotation).
- Ligament: Deltoid ligament.
- Rare due to strength of the ligament; often accompanied by avulsion fracture of the medial malleolus.
- Syndesmotic Sprain (“High Ankle Sprain”):
- Mechanism: Dorsiflexion + External rotation.
- Injury to the Anterior Inferior Tibiofibular Ligament (AITFL).
- Diagnostics: Ottawa Ankle Rules
- X-Ray Indicated ONLY if:
- Tenderness at posterior edge/tip of Lateral or Medial Malleolus.
- Tenderness at Base of 5th Metatarsal or Navicular.
- Inability to bear weight (4 steps immediately & in ED).
- Physical Exam
- Anterior Drawer: Tests ATFL.
- Talar Tilt: Tests CFL.
- Squeeze Test: Tests Syndesmosis.
- Treatment
- RICE (Rest, Ice, Compression, Elevation), NSAIDs.
- Early mobilization (weight-bearing as tolerated) > immobilization.
- High-Yield Associations
- Maisonneuve Fx: Proximal fibula fx associated with medial ankle injury. Always palpate proximal fibula.
- Jones Fx: Fracture at base of 5th metatarsal (risk of nonunion due to watershed blood supply).